Potrebbero piacerti anche
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- TB MeningitisDocumento17 pagineTB MeningitisSylvan LaminaNessuna valutazione finora
- AnorectalmalformationDocumento126 pagineAnorectalmalformationNinaNessuna valutazione finora
- MeningitisDocumento12 pagineMeningitisFaith Vaughn100% (2)
- Opthalmia UmDocumento23 pagineOpthalmia Umnanu-jenuNessuna valutazione finora
- Adrenal CrisisDocumento6 pagineAdrenal CrisisSteven SetioNessuna valutazione finora
- Case Study 2Documento37 pagineCase Study 2api-391842100Nessuna valutazione finora
- Bone Marrow ChecklistDocumento2 pagineBone Marrow ChecklistHasyim SuparlanNessuna valutazione finora
- Psychiatric EmergenciesDocumento25 paginePsychiatric EmergenciesAnnapurna DangetiNessuna valutazione finora
- Bronchial AsthmaDocumento95 pagineBronchial AsthmaBrian BrownNessuna valutazione finora
- Medico Legal Issues in NursingDocumento17 pagineMedico Legal Issues in Nursingakinyemi loladeNessuna valutazione finora
- Disseminated Intravascular CoagulationDocumento2 pagineDisseminated Intravascular CoagulationVince100% (1)
- Patterns of Nursing Care Delivery in IndiaDocumento22 paginePatterns of Nursing Care Delivery in IndiaBinu JoshvaNessuna valutazione finora
- Treatment Aspects in Perioperative NursingDocumento51 pagineTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- Assignment On Burns 2Documento15 pagineAssignment On Burns 2Suby Beigh100% (2)
- Case Study About: Cardiac Failure and Pulmonary EdemaDocumento32 pagineCase Study About: Cardiac Failure and Pulmonary EdemaIan Simon DorojaNessuna valutazione finora
- Standard Precautions PolicyDocumento8 pagineStandard Precautions PolicyMasrov TukirovNessuna valutazione finora
- Care of Unconscious PatientDocumento6 pagineCare of Unconscious PatientSuparna SinghaNessuna valutazione finora
- NephritisDocumento21 pagineNephritisruchikaNessuna valutazione finora
- Cardio Pulmonary Resuscitation and End of Life CareDocumento22 pagineCardio Pulmonary Resuscitation and End of Life CareAnitha sujithNessuna valutazione finora
- Renal CancerDocumento34 pagineRenal CancerArya100% (1)
- Laryngeal Cancer Powerpoint FinalllllDocumento30 pagineLaryngeal Cancer Powerpoint Finalllllapi-396575125Nessuna valutazione finora
- Neonatus - HIEDocumento24 pagineNeonatus - HIEAngeline AdrianneNessuna valutazione finora
- TurpDocumento23 pagineTurpColeen Comelle HuertoNessuna valutazione finora
- Presentation1 Cervical BiopsyDocumento14 paginePresentation1 Cervical BiopsyChanta MaharjanNessuna valutazione finora
- B M W M: IO Edical Aste AnagementDocumento23 pagineB M W M: IO Edical Aste AnagementJishnu JohnNessuna valutazione finora
- CervicitisDocumento7 pagineCervicitisElaisa Mae Delos SantosNessuna valutazione finora
- Nephrotic SyndromeDocumento28 pagineNephrotic Syndromerupali khillareNessuna valutazione finora
- Nephrotic SyndromeeDocumento28 pagineNephrotic SyndromeeRiteka SinghNessuna valutazione finora
- Bone Tumor: A. Nithya 1 Year M.SC (Nursing)Documento46 pagineBone Tumor: A. Nithya 1 Year M.SC (Nursing)nithya nithyaNessuna valutazione finora
- Hemodynamic MonitoringDocumento4 pagineHemodynamic Monitoringgurneet kourNessuna valutazione finora
- Choriocarcinoma 11Documento23 pagineChoriocarcinoma 11Fakhir HasanNessuna valutazione finora
- Acute Myeloid LeukemiaDocumento3 pagineAcute Myeloid LeukemiaKathleen Marie ChuangNessuna valutazione finora
- Congestive Cardiac FailureDocumento20 pagineCongestive Cardiac FailureAnand VaghasiyaNessuna valutazione finora
- Trends & Issues in MSN NursingDocumento41 pagineTrends & Issues in MSN NursingRajesh Sharma100% (3)
- Esophageal CancerDocumento25 pagineEsophageal CancerK poojithaNessuna valutazione finora
- Care of HemophiliaDocumento7 pagineCare of HemophiliaBasant karn100% (4)
- Health Problems MyselfDocumento54 pagineHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Approach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Documento6 pagineApproach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Suthar Keval CNessuna valutazione finora
- Common Health Problems of Infancy PowptDocumento78 pagineCommon Health Problems of Infancy PowptCiella Dela CruzNessuna valutazione finora
- Geriatric Considerations in Nursing: Priyanka. T M SC Nursing 1 YearDocumento70 pagineGeriatric Considerations in Nursing: Priyanka. T M SC Nursing 1 Yearsanthiyasandy100% (1)
- Respiratory Distress SyndromeDocumento41 pagineRespiratory Distress Syndromef.abrahamNessuna valutazione finora
- Cardiovascular and Thoracic NursingDocumento4 pagineCardiovascular and Thoracic NursingShreyas Walvekar100% (1)
- First Referral UnitDocumento24 pagineFirst Referral Unitjay5ar5jamorabon5torNessuna valutazione finora
- Diagnosi S: MalariaDocumento28 pagineDiagnosi S: MalariaOm Prakash SinghNessuna valutazione finora
- Antepartum HemorrhageDocumento5 pagineAntepartum Hemorrhagecode-24Nessuna valutazione finora
- Nursing Care PneumoniaDocumento26 pagineNursing Care PneumoniaIsaac Kipkemoi100% (1)
- Nursing - Academic CalendarDocumento4 pagineNursing - Academic CalendarKavi rajputNessuna valutazione finora
- Hypospadias and Epispadias 1Documento35 pagineHypospadias and Epispadias 1Corey100% (1)
- A Study To Assess The Effectiveness of Planned Teaching Program Regarding The Knowledge of Psycho Active Substance Abuse and Its Consequences On General Health Among The College STDocumento5 pagineA Study To Assess The Effectiveness of Planned Teaching Program Regarding The Knowledge of Psycho Active Substance Abuse and Its Consequences On General Health Among The College STInternational Journal of Innovative Science and Research Technology100% (1)
- DR Soni Rani, PGT Katihar Medical College, KatiharDocumento59 pagineDR Soni Rani, PGT Katihar Medical College, KatiharRamniwasMahoreNessuna valutazione finora
- Management Seminar - 2Documento27 pagineManagement Seminar - 2Esha KuttiNessuna valutazione finora
- Use of Computers in Teaching, Learning, Research & Nursing PracticeDocumento24 pagineUse of Computers in Teaching, Learning, Research & Nursing PracticeStephy SojanNessuna valutazione finora
- Hypertrophic Pyloric StenosisDocumento3 pagineHypertrophic Pyloric StenosisCandice ChengNessuna valutazione finora
- Neurological AssessmentDocumento5 pagineNeurological AssessmentVIDYANessuna valutazione finora
- Lymphoma in ChildrenDocumento42 pagineLymphoma in ChildrenPriyaNessuna valutazione finora
- First Aid Management For Falls and HangingDocumento4 pagineFirst Aid Management For Falls and HangingAnn Merlin JobinNessuna valutazione finora
- Nursing Care of Head InjuryDocumento1 paginaNursing Care of Head InjuryRaveen mayiNessuna valutazione finora
- Hiv and Aids in ChildrenDocumento36 pagineHiv and Aids in ChildrenKazau FwalangaNessuna valutazione finora
- Pain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityDocumento11 paginePain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityNilakshi Barik MandalNessuna valutazione finora
- Implanon: Subdermal Single Rod Contraceptive ImplantDocumento4 pagineImplanon: Subdermal Single Rod Contraceptive ImplantNilakshi Barik MandalNessuna valutazione finora
- Examination of The Breast: 11/14/2011 © Clinical Skills Resource Centre, University of Liverpool, UKDocumento19 pagineExamination of The Breast: 11/14/2011 © Clinical Skills Resource Centre, University of Liverpool, UKNilakshi Barik MandalNessuna valutazione finora
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocumento112 pagineClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNessuna valutazione finora
- Birth Injuries in Neonates: Pediatrics in Review November 2016Documento15 pagineBirth Injuries in Neonates: Pediatrics in Review November 2016Nilakshi Barik MandalNessuna valutazione finora
- Cardio Pulmonary Resuscitation Adult & Paediatric Definition of Cardiac ArrestDocumento8 pagineCardio Pulmonary Resuscitation Adult & Paediatric Definition of Cardiac ArrestNilakshi Barik Mandal0% (1)
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocumento112 pagineClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNessuna valutazione finora
- New Format With Correct LayoutDocumento3 pagineNew Format With Correct LayoutNilakshi Barik MandalNessuna valutazione finora
- Physical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NDocumento41 paginePhysical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NNilakshi Barik MandalNessuna valutazione finora
- Presented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowDocumento93 paginePresented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowNilakshi Barik MandalNessuna valutazione finora
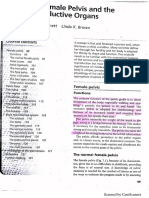
- Female PelvisDocumento7 pagineFemale PelvisNilakshi Barik MandalNessuna valutazione finora
- PreconceptionDocumento29 paginePreconceptionNilakshi Barik MandalNessuna valutazione finora
- Ijshr0038 PDFDocumento9 pagineIjshr0038 PDFNilakshi Barik MandalNessuna valutazione finora
- Gate Control TheoryDocumento6 pagineGate Control TheoryNilakshi Barik MandalNessuna valutazione finora
- Ms. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesDocumento11 pagineMs. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesNilakshi Barik MandalNessuna valutazione finora
- Gate Contro L Theory: Ms - Nilakshi Barik MandalDocumento6 pagineGate Contro L Theory: Ms - Nilakshi Barik MandalNilakshi Barik MandalNessuna valutazione finora
- History and Physical Assessment of Integumentary System: Mrs - Nilakshi Barik LecturerDocumento84 pagineHistory and Physical Assessment of Integumentary System: Mrs - Nilakshi Barik LecturerNilakshi Barik MandalNessuna valutazione finora
- Pain Manage Me NT: Ms - Nilakshi Barik MandalDocumento14 paginePain Manage Me NT: Ms - Nilakshi Barik MandalNilakshi Barik MandalNessuna valutazione finora
- Unit Plan For I Year BSC Nursing NUTRITION BATCH 2019-2020: Total Hours:60 HrsDocumento1 paginaUnit Plan For I Year BSC Nursing NUTRITION BATCH 2019-2020: Total Hours:60 HrsNilakshi Barik MandalNessuna valutazione finora
- Fetal SkullDocumento5 pagineFetal SkullNilakshi Barik MandalNessuna valutazione finora
- Preconception CouncellDocumento48 paginePreconception CouncellNilakshi Barik MandalNessuna valutazione finora
- In Partial Fulfillment of Requirement For The Degree of M: Fort, Bengaluru-560 002Documento128 pagineIn Partial Fulfillment of Requirement For The Degree of M: Fort, Bengaluru-560 002Nilakshi Barik MandalNessuna valutazione finora
- PostnatalcareguidelinesDocumento73 paginePostnatalcareguidelinesNilakshi Barik MandalNessuna valutazione finora
- Q.P. CODE 1764 Question Bank For Ii Year B.SC Nursing Community Health Nursing-I Unit-I Short Answers (2 Marks)Documento22 pagineQ.P. CODE 1764 Question Bank For Ii Year B.SC Nursing Community Health Nursing-I Unit-I Short Answers (2 Marks)Nilakshi Barik Mandal100% (1)
- Infertility: Presented ByDocumento47 pagineInfertility: Presented ByNilakshi Barik MandalNessuna valutazione finora
- Sampling Process in ResearchDocumento18 pagineSampling Process in ResearchNilakshi Barik MandalNessuna valutazione finora
- Permanent Contraception Method of Male (Vasectomy)Documento20 paginePermanent Contraception Method of Male (Vasectomy)Nilakshi Barik MandalNessuna valutazione finora
- Type of Question No. Unit NO. Topics Long Essay 10 Marks: Communication and Education Technology Layout QP 1765Documento1 paginaType of Question No. Unit NO. Topics Long Essay 10 Marks: Communication and Education Technology Layout QP 1765Nilakshi Barik MandalNessuna valutazione finora
- Sleep & Rest: Mr. M. Shivanandha ReddyDocumento59 pagineSleep & Rest: Mr. M. Shivanandha ReddyNilakshi Barik MandalNessuna valutazione finora
- Nursing Foundations-Basic BSC Nursing I Year Question Bank: Unit I Short AnswersDocumento10 pagineNursing Foundations-Basic BSC Nursing I Year Question Bank: Unit I Short AnswersNilakshi Barik MandalNessuna valutazione finora
- Antonovsky (1979)Documento280 pagineAntonovsky (1979)M.Fakhrul Kurnia100% (1)
- Mapeh 9 AssessmentDocumento4 pagineMapeh 9 AssessmentElmer John De LeonNessuna valutazione finora
- Pe 11 Modules 2Documento120 paginePe 11 Modules 2Martha Grace GrengiaNessuna valutazione finora
- Awareness On Lifestyle Diseases Among Adults of KeralaDocumento3 pagineAwareness On Lifestyle Diseases Among Adults of Keralachristy kurianNessuna valutazione finora
- English Analysing Themes and Ideas Presentation Beige Pink Lined StyleDocumento14 pagineEnglish Analysing Themes and Ideas Presentation Beige Pink Lined StylejrdccuevasNessuna valutazione finora
- Mongolia Pharma ReportDocumento38 pagineMongolia Pharma ReportphamleminhNessuna valutazione finora
- Print Version Vol 17 No 845Documento52 paginePrint Version Vol 17 No 845Henizion100% (1)
- WHO 2019 nCoV Therapeutics 2022.4 EngDocumento142 pagineWHO 2019 nCoV Therapeutics 2022.4 Engelsie versieNessuna valutazione finora
- Lec 2-Methods of PsychologyDocumento19 pagineLec 2-Methods of Psychologyrazaa0300Nessuna valutazione finora
- 3 s2.0 B9781455748013003301 MainDocumento120 pagine3 s2.0 B9781455748013003301 MainInzamam Ul HaqNessuna valutazione finora
- Prophylactic and Therapeutic Approach in Unani Medicine To Counter The Covid19 A ReviewDocumento8 pagineProphylactic and Therapeutic Approach in Unani Medicine To Counter The Covid19 A Reviewdr Shariq KhanNessuna valutazione finora
- Fortis Annual Report 2015 PDFDocumento320 pagineFortis Annual Report 2015 PDFProdigal SonNessuna valutazione finora
- Chapter 4 Non Infectious DiseasesDocumento32 pagineChapter 4 Non Infectious DiseasesLove IsNessuna valutazione finora
- Discussion: Cardiovascular Disease Mini-Case Study Case Study #2 Cardiovascular DiseaseDocumento3 pagineDiscussion: Cardiovascular Disease Mini-Case Study Case Study #2 Cardiovascular Diseaseapi-546898544Nessuna valutazione finora
- Drugs and Magic Remedies Act and Issues in AdvertisingDocumento13 pagineDrugs and Magic Remedies Act and Issues in Advertisingphani's100% (1)
- The Party Who Secures The Opinion of A Third Doctor: Further ReadingDocumento21 pagineThe Party Who Secures The Opinion of A Third Doctor: Further ReadingLyssa TabbuNessuna valutazione finora
- Pattern 6A: Primary Prevention/Risk Reduction For Cardiovascular/Pulmonary DisordersDocumento41 paginePattern 6A: Primary Prevention/Risk Reduction For Cardiovascular/Pulmonary DisordersClara Muñoz PiscoyaNessuna valutazione finora
- Chemical Risk Assessment 2013 1 Copy 1 PDFDocumento3 pagineChemical Risk Assessment 2013 1 Copy 1 PDFShekel Denino100% (1)
- Somatoform DisordersDocumento40 pagineSomatoform Disordersamal abdulrahmanNessuna valutazione finora
- Patient Centered in Heart Failure PatientsDocumento10 paginePatient Centered in Heart Failure PatientsberylianamayaNessuna valutazione finora
- Non Verbal LearningDocumento25 pagineNon Verbal LearningDruga DanutNessuna valutazione finora
- Money and The Law of AttractionDocumento4 pagineMoney and The Law of AttractionJack KrenzNessuna valutazione finora
- Report PDFDocumento7 pagineReport PDFBrayla WoolfolkNessuna valutazione finora
- Comman Line-1Documento20 pagineComman Line-1Prapti RakhasiaNessuna valutazione finora
- Updated HRRDA-final PDFDocumento64 pagineUpdated HRRDA-final PDFMa. Cristina MacaraigNessuna valutazione finora
- The Intersection Between Forensic Anthropometry and Cellular Physiology For Investigations: Prospects in Low and Middle-Income CountriesDocumento13 pagineThe Intersection Between Forensic Anthropometry and Cellular Physiology For Investigations: Prospects in Low and Middle-Income CountriesIJAR JOURNALNessuna valutazione finora
- Common Verbs For Health and Medical Treatment 2020Documento2 pagineCommon Verbs For Health and Medical Treatment 2020Gustavo ChucoNessuna valutazione finora
- FANGON - Module 3 Lesson 2 Activity 1Documento1 paginaFANGON - Module 3 Lesson 2 Activity 1Ella Nika FangonNessuna valutazione finora
- Multiple SclerosisDocumento35 pagineMultiple SclerosisJc SeguiNessuna valutazione finora
- IGNOU Block 1 Unit 1 Concepts of Community HealthDocumento17 pagineIGNOU Block 1 Unit 1 Concepts of Community Healtherice.research100% (1)