Potrebbero piacerti anche
- The ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryDa EverandThe ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryNessuna valutazione finora
- IHDI Ortho Presentation WebDocumento7 pagineIHDI Ortho Presentation WebC Martin TraumatoNessuna valutazione finora
- ScoliosisDocumento62 pagineScoliosisAbhinav Gupta0% (1)
- Isthmic Spondylolisthesis: Anterior Vs Posterior FusionDocumento48 pagineIsthmic Spondylolisthesis: Anterior Vs Posterior FusionneareastspineNessuna valutazione finora
- Overview Congenital Musculoskeletal DisorderDocumento84 pagineOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- SkeliosisDocumento55 pagineSkeliosisevelynNessuna valutazione finora
- ElastographyDocumento47 pagineElastographydoc0814Nessuna valutazione finora
- CtevDocumento30 pagineCtevHernanda Haudzan HakimNessuna valutazione finora
- Edu - DDH Final 19.5.07Documento27 pagineEdu - DDH Final 19.5.07Premnivas ParasuramanNessuna valutazione finora
- Hip ProblemsDocumento46 pagineHip ProblemsDhiya' VinaNessuna valutazione finora
- Abdominal Injury and Management: DR - MohammadzadehDocumento113 pagineAbdominal Injury and Management: DR - MohammadzadehDrArnab MohantyNessuna valutazione finora
- Screening 2Documento6 pagineScreening 2Yariel AraujoNessuna valutazione finora
- Uterine ProlapseDocumento45 pagineUterine ProlapseAnusree AnusreervNessuna valutazione finora
- Scoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai BangkinangDocumento36 pagineScoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai Bangkinangwindy noviantyNessuna valutazione finora
- Developmental Hip Dysplasia and DislocationDocumento51 pagineDevelopmental Hip Dysplasia and Dislocationandi firdha restuwatiNessuna valutazione finora
- Gait Abnormalities Following Slipped CapitalDocumento8 pagineGait Abnormalities Following Slipped Capitalyarimar hoyosNessuna valutazione finora
- Breech Delivery Shoulder Dystocia: James W. Van Hook, MDDocumento21 pagineBreech Delivery Shoulder Dystocia: James W. Van Hook, MDMansa SrivastavaNessuna valutazione finora
- CongenitalDocumento43 pagineCongenitalxantheNessuna valutazione finora
- DDHDocumento38 pagineDDHSanjiv GoyalNessuna valutazione finora
- Pregnancylaboranddelivery DeliveryDocumento73 paginePregnancylaboranddelivery DeliveryAdolfo ErlisNessuna valutazione finora
- Breech Presentation 2020Documento73 pagineBreech Presentation 2020Max ZealNessuna valutazione finora
- Deslizamiento Epifisiario Femur OvidDocumento7 pagineDeslizamiento Epifisiario Femur Ovidnathalia_pastasNessuna valutazione finora
- Developmental Dysplasia of HipDocumento68 pagineDevelopmental Dysplasia of HipwildanmalikNessuna valutazione finora
- Blount's Disease: Unit 6 Assignment October 11, 2011 Kathryn Bonvillian Jillianne HartDocumento20 pagineBlount's Disease: Unit 6 Assignment October 11, 2011 Kathryn Bonvillian Jillianne HartAgnes NesiaNessuna valutazione finora
- Children: Perinatal Femoral Fracture: A Ten-Year Observational Case Series StudyDocumento7 pagineChildren: Perinatal Femoral Fracture: A Ten-Year Observational Case Series StudyStella Gracia OctaricaNessuna valutazione finora
- Developmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedDocumento37 pagineDevelopmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedAh ZhangNessuna valutazione finora
- 2 - Ivica Zalud - IUGR Bali 2012.ppt (Read-Only)Documento43 pagine2 - Ivica Zalud - IUGR Bali 2012.ppt (Read-Only)Azura MotovlogNessuna valutazione finora
- Degenerative Scoliosis Case Presentations and DebateDocumento38 pagineDegenerative Scoliosis Case Presentations and DebateneareastspineNessuna valutazione finora
- DMCN 13480Documento9 pagineDMCN 13480contoisaNessuna valutazione finora
- Spinal Deformities NewDocumento79 pagineSpinal Deformities Newapi-26159412100% (3)
- Developmental Dysplasia of The HipDocumento88 pagineDevelopmental Dysplasia of The HipFera MulidarNessuna valutazione finora
- ClubfootDocumento9 pagineClubfootLorebell100% (5)
- Preterm BreechDocumento38 paginePreterm Breechorin78Nessuna valutazione finora
- CHD 1sDocumento32 pagineCHD 1sLauNessuna valutazione finora
- Lower Extremity DisordersDocumento25 pagineLower Extremity DisordersJameson87Nessuna valutazione finora
- Developmental (Congenital) Dysplasia of The Hip. Natural History and Prevention LevelsDocumento19 pagineDevelopmental (Congenital) Dysplasia of The Hip. Natural History and Prevention LevelsMEDS easyNessuna valutazione finora
- PE 074 FAI With Joane Kemp Handout PDFDocumento7 paginePE 074 FAI With Joane Kemp Handout PDFFer NandoNessuna valutazione finora
- CPDDocumento14 pagineCPDmaezuNessuna valutazione finora
- CanaveseJPediatrOrthop A2010Documento9 pagineCanaveseJPediatrOrthop A2010Samuel SalvadorNessuna valutazione finora
- EcografieDocumento81 pagineEcografieandreeamadalinaNessuna valutazione finora
- Undesensus TestisDocumento28 pagineUndesensus TestisMiftahuljannah SudirmanNessuna valutazione finora
- Orthopedic Conditions in PaedsDocumento57 pagineOrthopedic Conditions in PaedsAsma AlamNessuna valutazione finora
- CDH Congenital Dislocation of The HipDocumento65 pagineCDH Congenital Dislocation of The HipAshu AshNessuna valutazione finora
- Obs & Gyne OSCE CasesDocumento58 pagineObs & Gyne OSCE CasesMegan BolduanNessuna valutazione finora
- Radha Antenatal Fetal Well Being1Documento32 pagineRadha Antenatal Fetal Well Being1Shaells JoshiNessuna valutazione finora
- Giagnosis and Management HipDocumento4 pagineGiagnosis and Management HipSzőcs OrsolyaNessuna valutazione finora
- Genu VarumDocumento2 pagineGenu VarumMeis Malirmasele100% (1)
- Case Study PHDDocumento42 pagineCase Study PHDJoy AntonetteNessuna valutazione finora
- Yes, Materi 16 Januari 2013Documento42 pagineYes, Materi 16 Januari 2013Hendra SetyawanNessuna valutazione finora
- JournalclubpresentationDocumento31 pagineJournalclubpresentationrubinarashmi16Nessuna valutazione finora
- 5 The Pattern and Technique in The Clinical Evaluation of The Adult Hip The Common Physical Examination Tests of Hip Specialists 1353528420Documento12 pagine5 The Pattern and Technique in The Clinical Evaluation of The Adult Hip The Common Physical Examination Tests of Hip Specialists 1353528420César ArveláezNessuna valutazione finora
- Tibia Vara: ObjectivesDocumento3 pagineTibia Vara: ObjectivesJuan Carlos FigueroaNessuna valutazione finora
- Kyphosis Lordosis Defined This Drawing Represents The Spinal Condition ofDocumento36 pagineKyphosis Lordosis Defined This Drawing Represents The Spinal Condition ofSoare Elena-CosminaNessuna valutazione finora
- Clubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)Documento87 pagineClubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)muthia saniNessuna valutazione finora
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Documento73 pagineDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Muhamad Agung SupriyantoNessuna valutazione finora
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedDocumento73 pagineDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedMuhamad Agung SupriyantoNessuna valutazione finora
- Radiology of Obstetrics and GynaecologyDocumento61 pagineRadiology of Obstetrics and GynaecologyMUBIRU SAMUEL EDWARDNessuna valutazione finora
- Changes in The Sagittal Cranio-Cervical Posture Following A 12-Week Intervention Using A Simple Spinal Traction DeviceDocumento18 pagineChanges in The Sagittal Cranio-Cervical Posture Following A 12-Week Intervention Using A Simple Spinal Traction Device박진영Nessuna valutazione finora
- Rehabilitation of Scoliosis - Solo Final 6-10Documento30 pagineRehabilitation of Scoliosis - Solo Final 6-10Hanna RikaswaniNessuna valutazione finora
- Blount Disease - ASADocumento26 pagineBlount Disease - ASAMulya ImansyahNessuna valutazione finora
- Behaviour PAIN ASSESS PBRSDocumento12 pagineBehaviour PAIN ASSESS PBRSintannyNessuna valutazione finora
- A Guide To Undertanding Cerebral Palsy PDFDocumento32 pagineA Guide To Undertanding Cerebral Palsy PDFdisasatrianiNessuna valutazione finora
- Ask Hip SurveillanceDocumento26 pagineAsk Hip SurveillanceintannyNessuna valutazione finora
- Cpqol: Cerebral Palsy Quality of Life - ManualDocumento26 pagineCpqol: Cerebral Palsy Quality of Life - ManualintannyNessuna valutazione finora
- Barry Albright Dystonia ScaleDocumento3 pagineBarry Albright Dystonia Scaleintanny67% (3)
- Preliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureDocumento4 paginePreliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureCesar AlvearNessuna valutazione finora
- Foundation of Professional Nursing PracticeDocumento15 pagineFoundation of Professional Nursing PracticeArnie Jude CaridoNessuna valutazione finora
- Single Radius Clinical Research BrochureDocumento152 pagineSingle Radius Clinical Research BrochureВиктор ВасилевNessuna valutazione finora
- Surgical Anatomy of The Direct Anterior Approach For Total Hip ArthroplastyDocumento6 pagineSurgical Anatomy of The Direct Anterior Approach For Total Hip ArthroplastyFabio Sales VieiraNessuna valutazione finora
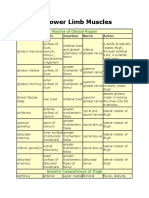
- Lower Limb MusclesDocumento8 pagineLower Limb Musclesbilal_kmu020% (1)
- Cavilha DFN SynthesDocumento26 pagineCavilha DFN SynthesSandra OliveiraNessuna valutazione finora
- Revision LCCK Instrumentation Surgical TechniqueDocumento112 pagineRevision LCCK Instrumentation Surgical TechniqueJehannah Dayanara HayudiniNessuna valutazione finora
- Case Study - CharleinDocumento13 pagineCase Study - Charleinmacky_lumberaNessuna valutazione finora
- The Menisci - A Comprehensive Review of Their Anatomy, Biomechanical Function and Surgical TreatmentDocumento197 pagineThe Menisci - A Comprehensive Review of Their Anatomy, Biomechanical Function and Surgical TreatmentYasmin100% (3)
- Anterior Cruciate Ligament Injury, Patient Variables, Outcomes and Knee OsteoarthritisDocumento135 pagineAnterior Cruciate Ligament Injury, Patient Variables, Outcomes and Knee OsteoarthritisNeutrino Fermi100% (1)
- Journal of Biomechanics: K.S. Halonen, M.E. Mononen, J.S. Jurvelin, J. To ̈yräs, J. Salo, R.K. KorhonenDocumento8 pagineJournal of Biomechanics: K.S. Halonen, M.E. Mononen, J.S. Jurvelin, J. To ̈yräs, J. Salo, R.K. KorhonenNikola MijailovićNessuna valutazione finora
- Anatomy and PhysiologyDocumento4 pagineAnatomy and PhysiologyAnnileighjeanNessuna valutazione finora
- ANATOMYDocumento9 pagineANATOMYAndrassy Twinkle AlineaNessuna valutazione finora
- Trauma CatalogueDocumento89 pagineTrauma Catalogueeshaputra100% (1)
- Zimmer Nexgen LCCK Surgical TechniqueDocumento27 pagineZimmer Nexgen LCCK Surgical TechniqueTudor MadalinaNessuna valutazione finora
- The Back of The Thigh & Popliteal Fossa-Tutorial PDFDocumento17 pagineThe Back of The Thigh & Popliteal Fossa-Tutorial PDFChipego ChiyaamaNessuna valutazione finora
- Persona The Personalized Knee Surgical TechniqueDocumento76 paginePersona The Personalized Knee Surgical TechniqueBIG JasonNessuna valutazione finora
- The Problem Knee 3rd Ed Hodder ArnoldDocumento262 pagineThe Problem Knee 3rd Ed Hodder Arnoldhasla16Nessuna valutazione finora
- Matching Nail Angle and Native Neck-Shaft AngleDocumento4 pagineMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNessuna valutazione finora
- Surgical Treatment of DDH in Adults, ThaDocumento11 pagineSurgical Treatment of DDH in Adults, ThaMyhay CretzuNessuna valutazione finora
- 17 Lower Extremity (FINAL)Documento32 pagine17 Lower Extremity (FINAL)kath-kath100% (1)
- Fractures of The HipDocumento198 pagineFractures of The HipPutri habna100% (1)
- Anatomy VivaDocumento5 pagineAnatomy Vivantege stuartNessuna valutazione finora
- Lower Limb RadiographyDocumento144 pagineLower Limb RadiographyMunish Dogra0% (1)
- AOTrauma Course-Advanced Principles of Fracture Management August 6-8, 2015, Kunming, ChinaDocumento20 pagineAOTrauma Course-Advanced Principles of Fracture Management August 6-8, 2015, Kunming, ChinafaluviekadianiNessuna valutazione finora
- Case Study - FractureDocumento58 pagineCase Study - FractureChristian97% (31)
- Chapter 3 Musculoskeletal Systems Part 2Documento106 pagineChapter 3 Musculoskeletal Systems Part 2kamalab04Nessuna valutazione finora
- ACL Reconstruction With Bone-Tendon-Bone Transplants Using The Endobutton CL BTB Fixation SystemDocumento12 pagineACL Reconstruction With Bone-Tendon-Bone Transplants Using The Endobutton CL BTB Fixation Systemapi-19808945Nessuna valutazione finora
- PACES 3 - AbdomenDocumento14 paginePACES 3 - AbdomenDrShamshad KhanNessuna valutazione finora
- Joints and Ligaments Anatomy TablesDocumento32 pagineJoints and Ligaments Anatomy TablessmoggindakrakNessuna valutazione finora