Potrebbero piacerti anche
- IIITDM Yoga HandbookDocumento24 pagineIIITDM Yoga HandbookBenoit HsuNessuna valutazione finora
- Adverse Reaction To DrugsDocumento22 pagineAdverse Reaction To DrugssridharNessuna valutazione finora
- Lower Limb Evaluation Format Lower Limb Fracture Assesstment FormDocumento12 pagineLower Limb Evaluation Format Lower Limb Fracture Assesstment FormsridharNessuna valutazione finora
- Guidelines For Pre Submission Seminar-LPUDocumento1 paginaGuidelines For Pre Submission Seminar-LPUsridharNessuna valutazione finora
- Liver Enzymes (AST-ALT)Documento3 pagineLiver Enzymes (AST-ALT)sridharNessuna valutazione finora
- Brachial Plexus InjuryDocumento43 pagineBrachial Plexus InjurysridharNessuna valutazione finora
- Patterns of PNFDocumento39 paginePatterns of PNFsridhar100% (1)
- 01-13 2 End Diastolic Pneumatic Compression Boot As A Treatment of PVD or LymphedemaDocumento4 pagine01-13 2 End Diastolic Pneumatic Compression Boot As A Treatment of PVD or LymphedemasridharNessuna valutazione finora
- Hepatitis B VirusDocumento47 pagineHepatitis B VirusDiah Puspita RiniNessuna valutazione finora
- 10-11 Gbs General Neuro 2nd YearDocumento29 pagine10-11 Gbs General Neuro 2nd YearsridharNessuna valutazione finora
- PNFDocumento39 paginePNFsridhar100% (1)
- Nerve Conduction Velocity StudiesDocumento12 pagineNerve Conduction Velocity StudiessridharNessuna valutazione finora
- Thoracic Spine AnatomyDocumento5 pagineThoracic Spine AnatomysridharNessuna valutazione finora
- Brachial Plexus InjuryDocumento43 pagineBrachial Plexus InjurysridharNessuna valutazione finora
- Ankle MobilizationDocumento16 pagineAnkle MobilizationsridharNessuna valutazione finora
- Sudden Infant Death SyndromeDocumento20 pagineSudden Infant Death SyndromesridharNessuna valutazione finora
- Inflammatory My Opa ThiesDocumento10 pagineInflammatory My Opa ThiessridharNessuna valutazione finora
- Imaging Findings and Clinical Correlation: Cerebral Herniation SyndromesDocumento64 pagineImaging Findings and Clinical Correlation: Cerebral Herniation SyndromessridharNessuna valutazione finora
- Brachial Plexus InjuryDocumento43 pagineBrachial Plexus InjurysridharNessuna valutazione finora
- Imaging Findings and Clinical Correlation: Cerebral Herniation SyndromesDocumento64 pagineImaging Findings and Clinical Correlation: Cerebral Herniation SyndromessridharNessuna valutazione finora
- Tardieu ScaleDocumento2 pagineTardieu ScalesridharNessuna valutazione finora
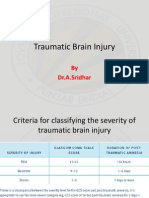
- Traumatic Brain InjuryDocumento26 pagineTraumatic Brain InjurysridharNessuna valutazione finora
- Infra RedDocumento7 pagineInfra RedsridharNessuna valutazione finora
- Application FormatDocumento2 pagineApplication FormatsridharNessuna valutazione finora
- Windlass Effect Ankle JointDocumento35 pagineWindlass Effect Ankle JointsridharNessuna valutazione finora
- Vinayagar Agaval - Avvaiyar PDFDocumento17 pagineVinayagar Agaval - Avvaiyar PDFkckejaman100% (1)
- Skanda Shasti KavachamDocumento6 pagineSkanda Shasti KavachamsriramanaNessuna valutazione finora
- College of NursingDocumento1 paginaCollege of NursingsridharNessuna valutazione finora
- Clavicle FractureDocumento4 pagineClavicle FracturesridharNessuna valutazione finora
- Clavicle FractureDocumento9 pagineClavicle FracturesridharNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cunningham & Turner, 2016Documento38 pagineCunningham & Turner, 2016Ratu SetiawanNessuna valutazione finora
- Manufacturing process F1 racing car proposalDocumento4 pagineManufacturing process F1 racing car proposalFirdaus IliasNessuna valutazione finora
- Demonstration and Mechanism of Brudzinski and KernDocumento3 pagineDemonstration and Mechanism of Brudzinski and KernYamamoto YuichiNessuna valutazione finora
- STLTKD HandbookDocumento34 pagineSTLTKD HandbookMark De JesusNessuna valutazione finora
- Discover 135 DTSiPart Catalogue PDFDocumento46 pagineDiscover 135 DTSiPart Catalogue PDFDZ50% (2)
- 722.9 Tranmission ServiceDocumento3 pagine722.9 Tranmission ServiceKISKACNessuna valutazione finora
- Unit 6 WKST 4 Answer Key RevDocumento3 pagineUnit 6 WKST 4 Answer Key RevTushar Raj83% (6)
- EVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFDocumento1 paginaEVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFArrafi FahrezaNessuna valutazione finora
- Siyensikula Script Not Yet CompleteDocumento2 pagineSiyensikula Script Not Yet CompleteJ AblangNessuna valutazione finora
- Reps: Means That How Much You Do Each Time Sets: Example 20 Reps 1 SetDocumento2 pagineReps: Means That How Much You Do Each Time Sets: Example 20 Reps 1 SetHarry MiglaniNessuna valutazione finora
- Seville Car SeatDocumento16 pagineSeville Car SeatSherif HassanNessuna valutazione finora
- Construction and Working:: Porter GovernorDocumento5 pagineConstruction and Working:: Porter Governoraverify53Nessuna valutazione finora
- Exercies For Lower BackDocumento2 pagineExercies For Lower BackAnkush RatanpalNessuna valutazione finora
- Season3 PKL DATA FOR DATA ANALYTICSDocumento3 pagineSeason3 PKL DATA FOR DATA ANALYTICSBhagya SreeNessuna valutazione finora
- Beer Pong Table DesignDocumento5 pagineBeer Pong Table DesignMatt JohnsonNessuna valutazione finora
- Link Volkswagen GolDocumento11 pagineLink Volkswagen GolDiego De La Fuente0% (1)
- PriceList 201120Documento1 paginaPriceList 201120KorRhinoNessuna valutazione finora
- Electrical Resistant Heavy Duty Safety Shoes With MidsoleDocumento3 pagineElectrical Resistant Heavy Duty Safety Shoes With MidsoleEunice GayetaNessuna valutazione finora
- Shred ProgramDocumento12 pagineShred ProgramLayke CrosslandNessuna valutazione finora
- Monetizing Casual Games The Right Way (Ebook by Appodeal)Documento16 pagineMonetizing Casual Games The Right Way (Ebook by Appodeal)roleplay_brNessuna valutazione finora
- SupercarDocumento3 pagineSupercarsigne.soderstrom1785Nessuna valutazione finora
- Sector 3 Built Up HouseDocumento36 pagineSector 3 Built Up Housekksingh007india0% (1)
- Clinical Oriented Anatomy of Urinary SystemDocumento81 pagineClinical Oriented Anatomy of Urinary SystemRizcky Naldy Eka Putra100% (1)
- BigMex - Manage BlogDocumento6 pagineBigMex - Manage Blogfei biouNessuna valutazione finora
- Leading-Edge Motorsport Technology Since 1990Documento22 pagineLeading-Edge Motorsport Technology Since 1990tushar girotra100% (1)
- Amber Alert: Issued by Texas Dept. of Public SafetyDocumento2 pagineAmber Alert: Issued by Texas Dept. of Public SafetyBrandon ScottNessuna valutazione finora
- Handball Basics PDFDocumento13 pagineHandball Basics PDFyunzhe hanNessuna valutazione finora
- Geo StormDocumento5 pagineGeo StormRoberto Ortega MicalizziNessuna valutazione finora
- 12-Pe Question Bank - Physical Education - Class - 12Documento17 pagine12-Pe Question Bank - Physical Education - Class - 12Fire FlamesNessuna valutazione finora