Potrebbero piacerti anche
- Affidavit identityDocumento4 pagineAffidavit identityNeill Matthew Addison Ortiz54% (13)
- Healing VisualisationDocumento180 pagineHealing Visualisationsol suna100% (3)
- Doctor's Order Phase 2Documento5 pagineDoctor's Order Phase 2Renea Joy ArruejoNessuna valutazione finora
- Cancer DiseaseDocumento7 pagineCancer Diseasenbs saraswathiNessuna valutazione finora
- RLE Clinical RotationDocumento2 pagineRLE Clinical RotationtwothumbsNessuna valutazione finora
- Konsulta Key ProcessDocumento9 pagineKonsulta Key ProcessArlo Winston De GuzmanNessuna valutazione finora
- Needle Stick Injury FormatDocumento1 paginaNeedle Stick Injury Formatquality qualityNessuna valutazione finora
- Antepartum Record Labor WatchDocumento4 pagineAntepartum Record Labor WatchMaryJoy rosalesNessuna valutazione finora
- Case Investigation Forms - Pidsrmop3ed 1Documento16 pagineCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Psychopharmacology For Mental Health Professionals An Integrative Approach 2nd Edition Ebook PDFDocumento62 paginePsychopharmacology For Mental Health Professionals An Integrative Approach 2nd Edition Ebook PDFpatrick.mcfadden11197% (38)
- Mapeh Grade 8 Third QuarterDocumento4 pagineMapeh Grade 8 Third QuarterPhilip Jansen Guarin100% (2)
- Case Investigation Form for AEFIDocumento4 pagineCase Investigation Form for AEFICHICKYNessuna valutazione finora
- Referral Form SummaryDocumento8 pagineReferral Form Summarycar3laNessuna valutazione finora
- Shrimp FarmingDocumento12 pagineShrimp FarmingGrowel Agrovet Private Limited.100% (2)
- Birthing Homes ReqDocumento10 pagineBirthing Homes ReqMi Lagro100% (2)
- Neuromuscular Blocking DrugsDocumento23 pagineNeuromuscular Blocking DrugsRA TranceNessuna valutazione finora
- Nurse Volunteer Job DescriptionDocumento1 paginaNurse Volunteer Job DescriptionEunice Culaway100% (1)
- Emergency and Disaster NursingDocumento13 pagineEmergency and Disaster Nursingkarenkaren09Nessuna valutazione finora
- Weekly Notifiable 2023Documento1 paginaWeekly Notifiable 2023johnmorts2014100% (1)
- Monthly Newborn Screening ReportDocumento1 paginaMonthly Newborn Screening ReportEarl Parungao50% (2)
- Firecracker Injury PreventionDocumento13 pagineFirecracker Injury PreventionRosie HajironNessuna valutazione finora
- Record pneumococcal vaccinationDocumento1 paginaRecord pneumococcal vaccinationalfredtan6288Nessuna valutazione finora
- PhilHealth Circular 2020-0021 Accreditation For Provision of Konsulta Package As Primary Care Benefit PackageDocumento7 paginePhilHealth Circular 2020-0021 Accreditation For Provision of Konsulta Package As Primary Care Benefit PackageJessa MaeNessuna valutazione finora
- ABC ProposalDocumento4 pagineABC ProposalsilveoNessuna valutazione finora
- Nursing Care Plan Preterm LaborDocumento3 pagineNursing Care Plan Preterm LaborAdriane Coma100% (1)
- Bhalaaji - Art and Science of Orthodontics WordDocumento578 pagineBhalaaji - Art and Science of Orthodontics WordBudi AthAnza Suhartono85% (13)
- Dengue NS1 RDT Annex 5-6Documento4 pagineDengue NS1 RDT Annex 5-6Ga B B Orlongan100% (1)
- DOH-Accredited OFW Clinics PDFDocumento12 pagineDOH-Accredited OFW Clinics PDFEda TenajerosNessuna valutazione finora
- Job Duties and Tasks For NursesDocumento9 pagineJob Duties and Tasks For NursesCzar Crio Ai Rosales100% (1)
- DengueDocumento2 pagineDengueTherence Marie LacsonNessuna valutazione finora
- Doh Exam CoverageDocumento3 pagineDoh Exam CoverageAlavitz Aslambert100% (1)
- Dermatitis and HomoeopathyDocumento18 pagineDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Nurse Deployment Programndp Examination NotesDocumento139 pagineNurse Deployment Programndp Examination NotesDechy Lyn PalmaNessuna valutazione finora
- Nurs 3020 - Erin Final EvaluationDocumento14 pagineNurs 3020 - Erin Final Evaluationapi-505854426Nessuna valutazione finora
- Assessment of RA 9994 implementation for senior citizensDocumento12 pagineAssessment of RA 9994 implementation for senior citizenserroljohnescorial100% (1)
- Post Anesthesia Care UnitDocumento10 paginePost Anesthesia Care UnitMaria Criselda C. CelonNessuna valutazione finora
- DENGUE-TASK-FORCE-SAMPLE-EO BarangayDocumento3 pagineDENGUE-TASK-FORCE-SAMPLE-EO BarangayCHICKY100% (8)
- CRF HFMD AsmghDocumento2 pagineCRF HFMD AsmghRyeowook RyeNessuna valutazione finora
- Measles CIF 2014Documento2 pagineMeasles CIF 2014RionaMarieMagbutayNessuna valutazione finora
- NTP Quarterly Report On Hospital TB Referrals RevisedDocumento1 paginaNTP Quarterly Report On Hospital TB Referrals RevisedMark Johnuel DuavisNessuna valutazione finora
- TB TX CertificationDocumento7 pagineTB TX CertificationReinald Raven GuerreroNessuna valutazione finora
- Reed Mod3 Assignment 3 Policies For Retention and Destruction of Health RecordsDocumento3 pagineReed Mod3 Assignment 3 Policies For Retention and Destruction of Health Recordsapi-340267228100% (1)
- ESR Verification Form ReviseDocumento4 pagineESR Verification Form ReviseRouella DoverteNessuna valutazione finora
- Updated DOH ProgramsDocumento37 pagineUpdated DOH ProgramsRaymund Christopher Dela PeñaNessuna valutazione finora
- EPI Teaching DemoDocumento32 pagineEPI Teaching DemoRommel G. Santiago100% (2)
- National TB Control Program Form 7 - Referral FormDocumento1 paginaNational TB Control Program Form 7 - Referral FormAre Pee EtcNessuna valutazione finora
- Ibajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianDocumento22 pagineIbajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianMary Jean GelitoNessuna valutazione finora
- Mariano Marcos State University: College of Health SciencesDocumento3 pagineMariano Marcos State University: College of Health SciencesJoshua GonzalesNessuna valutazione finora
- Rural Health Animal Bite FormDocumento1 paginaRural Health Animal Bite FormConcepcion RHUNessuna valutazione finora
- Activity Report Medical Mission Sept 20Documento11 pagineActivity Report Medical Mission Sept 20Krizelle Mae BaronganNessuna valutazione finora
- Monthly Report Form For NDP Edited 2 From PHTDocumento1 paginaMonthly Report Form For NDP Edited 2 From PHTAnthony Zuniega0% (1)
- FAQs For Health FacilitiesDocumento17 pagineFAQs For Health FacilitiesPhilhealth ISDH SinaitNessuna valutazione finora
- Assessment Tool For Level 1 Hospital Annex K1 PDFDocumento47 pagineAssessment Tool For Level 1 Hospital Annex K1 PDFMadelyn LamanilaoNessuna valutazione finora
- Nursing Care Hours Per Patient DayDocumento5 pagineNursing Care Hours Per Patient Dayjo_annamae4413Nessuna valutazione finora
- AFPMC Citizen's Charter GuideDocumento17 pagineAFPMC Citizen's Charter GuideMae Flor FuentespinaNessuna valutazione finora
- ICE Checklist #4: Cleaning and Disinfection of The Dialysis StationDocumento1 paginaICE Checklist #4: Cleaning and Disinfection of The Dialysis StationAbidi Hichem100% (2)
- Usap Tayo Sa FP Attendance SheetDocumento2 pagineUsap Tayo Sa FP Attendance SheetRan DyNessuna valutazione finora
- Affidavit Form Medical Clinic Fire SafetyDocumento2 pagineAffidavit Form Medical Clinic Fire SafetysrinivasuNessuna valutazione finora
- NLE 2010 Room Assignment - Legazpi ExamineesDocumento128 pagineNLE 2010 Room Assignment - Legazpi ExamineesLyle SantosNessuna valutazione finora
- NDP Monthly Journal February 2014 Calapan CityDocumento3 pagineNDP Monthly Journal February 2014 Calapan CityMenchie Vivas-Alot100% (1)
- 2023 (DRAFT) HESU Integrated Monitoring and Evaluation ToolDocumento21 pagine2023 (DRAFT) HESU Integrated Monitoring and Evaluation Toolcharles nikko sabinoNessuna valutazione finora
- Clinical Teaching Plan A. General Information: Related Learning ExperienceDocumento2 pagineClinical Teaching Plan A. General Information: Related Learning ExperienceGee RidadNessuna valutazione finora
- AOP-2024-narrative FINALDocumento66 pagineAOP-2024-narrative FINALjasper manuelNessuna valutazione finora
- PRD-07 Action Sheet For AuthenticationDocumento2 paginePRD-07 Action Sheet For AuthenticationMary CindyNessuna valutazione finora
- FOURmula OneDocumento15 pagineFOURmula Onejona phie Montero100% (1)
- Epidemiology 201 ReviewDocumento93 pagineEpidemiology 201 ReviewJillian AsdalaNessuna valutazione finora
- HWAP - ST Paul Hospital Tuguegarao CagayanDocumento33 pagineHWAP - ST Paul Hospital Tuguegarao CagayanDino SubingsubingNessuna valutazione finora
- Transfer Hospital Choice FormDocumento1 paginaTransfer Hospital Choice FormAina Haravata100% (1)
- Department of Health ProgramsDocumento14 pagineDepartment of Health ProgramsJan Kristel A. QuijanoNessuna valutazione finora
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Documento7 pagineCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNessuna valutazione finora
- Post-Exam Health Report FormDocumento1 paginaPost-Exam Health Report FormBricks JauNessuna valutazione finora
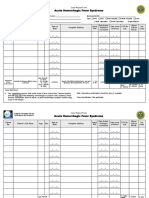
- Acute Hemorrhagic Fever - CRFDocumento1 paginaAcute Hemorrhagic Fever - CRFMary Anne Grace GarridoNessuna valutazione finora
- Acute Bloody Diarrhea - CRFDocumento2 pagineAcute Bloody Diarrhea - CRFMary Anne Grace Garrido0% (1)
- Philippine Disease Surveillance Report FormDocumento30 paginePhilippine Disease Surveillance Report FormAbigail Palig-adNessuna valutazione finora
- Acute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFDocumento2 pagineAcute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFCHICKYNessuna valutazione finora
- CRF TyphoidDocumento2 pagineCRF TyphoidAndria GuialalNessuna valutazione finora
- Climate Stimuli Impact on Population and Natural ResourcesDocumento48 pagineClimate Stimuli Impact on Population and Natural ResourcesCHICKYNessuna valutazione finora
- Step 3 - Exposure DatabaseDocumento19 pagineStep 3 - Exposure DatabaseCHICKYNessuna valutazione finora
- Step 5 - DRADocumento19 pagineStep 5 - DRACHICKYNessuna valutazione finora
- Step 2 Climate Change Projections and ImpactsDocumento6 pagineStep 2 Climate Change Projections and ImpactsCHICKYNessuna valutazione finora
- CCVA-CDRA AnnexesDocumento55 pagineCCVA-CDRA AnnexesCHICKYNessuna valutazione finora
- Affidavit IIDocumento2 pagineAffidavit IICHICKYNessuna valutazione finora
- R8 - Samar CLIRAM - NewDocumento4 pagineR8 - Samar CLIRAM - NewCHICKYNessuna valutazione finora
- CCVA-CDRA AnnexesDocumento55 pagineCCVA-CDRA AnnexesCHICKYNessuna valutazione finora
- Affidavit IIIDocumento2 pagineAffidavit IIICHICKYNessuna valutazione finora
- Decision Area/s (Barangay) Hazards/Problems Technical Findings Impacts/Implications Policy InterventionsDocumento2 pagineDecision Area/s (Barangay) Hazards/Problems Technical Findings Impacts/Implications Policy InterventionsCHICKYNessuna valutazione finora
- Intro To CDRADocumento51 pagineIntro To CDRACHICKYNessuna valutazione finora
- Health Certificate LogbookDocumento2 pagineHealth Certificate LogbookCHICKYNessuna valutazione finora
- Quotation: Attn: Ruth C. Nablo, RMT MHODocumento1 paginaQuotation: Attn: Ruth C. Nablo, RMT MHOCHICKYNessuna valutazione finora
- AMES Part 2 PDFDocumento1 paginaAMES Part 2 PDFCHICKYNessuna valutazione finora
- Summary CovidDocumento1 paginaSummary CovidCHICKYNessuna valutazione finora
- Acute Encephalitis Syndrome - Ver Oct 12 2012 PDFDocumento2 pagineAcute Encephalitis Syndrome - Ver Oct 12 2012 PDFCHICKYNessuna valutazione finora
- Dengue Update in Samar Province Surpasses Epidemic ThresholdDocumento10 pagineDengue Update in Samar Province Surpasses Epidemic ThresholdCHICKYNessuna valutazione finora
- YesDocumento1 paginaYesCHICKYNessuna valutazione finora
- Contact Tracing For LGUsDocumento21 pagineContact Tracing For LGUsCHICKYNessuna valutazione finora
- Acute Encephalitis Syndrome - Ver Oct 12 2012 PDFDocumento2 pagineAcute Encephalitis Syndrome - Ver Oct 12 2012 PDFCHICKYNessuna valutazione finora
- Acute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFDocumento2 pagineAcute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFCHICKYNessuna valutazione finora
- Barangay Monitoring ToolDocumento8 pagineBarangay Monitoring ToolCHICKYNessuna valutazione finora
- CHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDDocumento1 paginaCHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDCHICKYNessuna valutazione finora
- Self-Assessment Tool For Temporary Treatment & Monitoring Facilities For COVID-19Documento3 pagineSelf-Assessment Tool For Temporary Treatment & Monitoring Facilities For COVID-19CHICKYNessuna valutazione finora
- AMES Part 2 PDFDocumento1 paginaAMES Part 2 PDFCHICKYNessuna valutazione finora
- Peran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Documento31 paginePeran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Miftahul HudaNessuna valutazione finora
- MiconazoleDocumento3 pagineMiconazoleapi-3797941Nessuna valutazione finora
- Boards Garden Ph-2Documento32 pagineBoards Garden Ph-2Vijay KumarNessuna valutazione finora
- GliclazideDocumento5 pagineGliclazideGwyn RosalesNessuna valutazione finora
- Case PresentationDocumento22 pagineCase PresentationManjunath ArunachalamNessuna valutazione finora
- Daftar Pustaka KorneaDocumento3 pagineDaftar Pustaka KorneaMuhammad Apriliandy ShariffNessuna valutazione finora
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocumento5 pagineDiabetes & Metabolic Syndrome: Clinical Research & ReviewsPetra Diansari ZegaNessuna valutazione finora
- 3rd Ed General Cheat Sheet PDFDocumento9 pagine3rd Ed General Cheat Sheet PDFAlan RideoutNessuna valutazione finora
- AlkaloidsDocumento21 pagineAlkaloidssanjiv_m20100% (1)
- No Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanDocumento16 pagineNo Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanNurmalasari SaryNessuna valutazione finora
- Accepted Manuscript: Complementary Therapies in MedicineDocumento24 pagineAccepted Manuscript: Complementary Therapies in MedicineAndrea BarresiNessuna valutazione finora
- c1 04 Chua Va Dinh Huong Cau Hoi BTTL 5874Documento8 paginec1 04 Chua Va Dinh Huong Cau Hoi BTTL 5874Hoang SonNessuna valutazione finora
- Food Adulteration: A Review: March 2017Documento5 pagineFood Adulteration: A Review: March 2017Payal GandhiNessuna valutazione finora
- Biological Psychiatry: Is There Any Other KindDocumento9 pagineBiological Psychiatry: Is There Any Other KindLiam Jacque LapuzNessuna valutazione finora
- COMEDK PGET-2008 Answer KeysDocumento23 pagineCOMEDK PGET-2008 Answer Keysmobiled2Nessuna valutazione finora
- Pityriasis AlbaDocumento6 paginePityriasis AlbaLee Eng SiangNessuna valutazione finora
- Pathophysiology of Ectopic PregnancyDocumento11 paginePathophysiology of Ectopic PregnancyJann ericka JaoNessuna valutazione finora
- Judi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Documento66 pagineJudi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Judi Januadi Endjun, MD, ObsGynNessuna valutazione finora