Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cor Pulmonale ReDocumento35 pagineCor Pulmonale ReFabb NelsonNessuna valutazione finora
- Arteries & Veins, IGCSE, BiologyDocumento11 pagineArteries & Veins, IGCSE, BiologyyarinaosuNessuna valutazione finora
- Renal Blood Flow Regulation - Indd - Osmosis PDFDocumento3 pagineRenal Blood Flow Regulation - Indd - Osmosis PDFLana AmerieNessuna valutazione finora
- Seminar Electrocardiogram (ECG)Documento32 pagineSeminar Electrocardiogram (ECG)Jamuna PatelNessuna valutazione finora
- HCA220r4 Course SyllabusDocumento19 pagineHCA220r4 Course SyllabusAnnieNessuna valutazione finora
- Point-Of-Care Ultrasound in Cardiac ArrestDocumento13 paginePoint-Of-Care Ultrasound in Cardiac ArrestEgorSazhaevNessuna valutazione finora
- Myocardial Infarction With CABG Concept MapDocumento1 paginaMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- ECG Changes in Left Ventricular HypertrophyDocumento25 pagineECG Changes in Left Ventricular HypertrophyMuhammad AsifNessuna valutazione finora
- Alice in IntensivelandDocumento13 pagineAlice in IntensivelandPablo VélezNessuna valutazione finora
- Atrial Fibrillation and Atrial FlutterDocumento4 pagineAtrial Fibrillation and Atrial FlutterROHITNessuna valutazione finora
- Myocardial InfarctionDocumento15 pagineMyocardial Infarctionanon_877280340Nessuna valutazione finora
- Assessment of Cardiovascular SystemDocumento41 pagineAssessment of Cardiovascular Systembicariato100% (7)
- Chronic Venous Congestion of Lung, Liver and SpleenDocumento24 pagineChronic Venous Congestion of Lung, Liver and SpleenSanjana YadwadNessuna valutazione finora
- Medical Astrology - Medicine by The StarsDocumento4 pagineMedical Astrology - Medicine by The Starskrmass25Nessuna valutazione finora
- Making Sense of Exercise Testing PDFDocumento143 pagineMaking Sense of Exercise Testing PDFpylot100% (3)
- Biology As Level: Practise QuestionDocumento82 pagineBiology As Level: Practise QuestionTamanna AdibaNessuna valutazione finora
- Reading Unit 9 CardiologyDocumento4 pagineReading Unit 9 CardiologyChristian SilvaNessuna valutazione finora
- Blood Pressure LevelsDocumento4 pagineBlood Pressure LevelsHeart of the Valley, Pediatric CardiologyNessuna valutazione finora
- Intracardiac Epinephrine Injection During Open Thoracotomy and Circulatory ArrestDocumento2 pagineIntracardiac Epinephrine Injection During Open Thoracotomy and Circulatory ArrestRaven DelargeNessuna valutazione finora
- Ankle Brachial Index PDFDocumento8 pagineAnkle Brachial Index PDFIncredibleNessuna valutazione finora
- Program Book of INAechoDocumento15 pagineProgram Book of INAechoAnthomina MayaNessuna valutazione finora
- Sci 9 Q1 Module 1Documento22 pagineSci 9 Q1 Module 1John Merby GonzalesNessuna valutazione finora
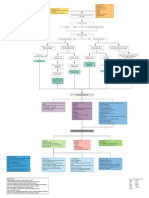
- Natriuretic Peptide SystemDocumento30 pagineNatriuretic Peptide SystemKhaled S. Harb100% (1)
- Presentor: DR - Kumar Moderator: DR - VamsidharDocumento71 paginePresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyNessuna valutazione finora
- Introduction To Human Anatomy and PhysiologyDocumento5 pagineIntroduction To Human Anatomy and PhysiologySam Raven AndresNessuna valutazione finora
- Heart and PericardiumDocumento26 pagineHeart and PericardiumpalNessuna valutazione finora
- Heart Failure in Dogs: 6 Practical Tips From CardiologistsDocumento6 pagineHeart Failure in Dogs: 6 Practical Tips From CardiologistsJessareth Atilano CapacioNessuna valutazione finora
- Pulse Rate LabDocumento2 paginePulse Rate LabGemini JuneboiNessuna valutazione finora
- Valvular Heart Disease IM 8-12 NewDocumento80 pagineValvular Heart Disease IM 8-12 NewRachilla Arandita SaraswatiNessuna valutazione finora
- ElectrocardiogramaDocumento6 pagineElectrocardiogramaMay GaamNessuna valutazione finora