Potrebbero piacerti anche
- Class 6 (19.07.2022)Documento70 pagineClass 6 (19.07.2022)Ãqûã FîggâNessuna valutazione finora
- Kuliah Hyper and Hypothyroid - 2014Documento66 pagineKuliah Hyper and Hypothyroid - 2014Clararida RiawanNessuna valutazione finora
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocumento7 pagineThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNessuna valutazione finora
- Im-Thyroid DisordersDocumento9 pagineIm-Thyroid DisordersRyan F. BernalNessuna valutazione finora
- Thyroid Function Tests: Understanding the Hidden Health ProblemDocumento34 pagineThyroid Function Tests: Understanding the Hidden Health Problemvjanand07100% (1)
- Talking Thyroid FactsDocumento6 pagineTalking Thyroid FactsVegan Future100% (4)
- CC 3-Lab FKM 17Documento4 pagineCC 3-Lab FKM 17mayabangkurtipotNessuna valutazione finora
- Clinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismDocumento69 pagineClinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismTutde SedanaNessuna valutazione finora
- Hyperthyroidism and HypothyroidismDocumento28 pagineHyperthyroidism and HypothyroidismAlthea AlbaniaNessuna valutazione finora
- Thyroid ReportDocumento105 pagineThyroid ReportAARVNessuna valutazione finora
- Hypothyroidism in PregnancyDocumento32 pagineHypothyroidism in PregnancyNicks KumarNessuna valutazione finora
- Disorders of Thyroid Gland - S.D Osuntoye-1Documento32 pagineDisorders of Thyroid Gland - S.D Osuntoye-1IiiNessuna valutazione finora
- HipertiroidDocumento37 pagineHipertiroidTaysqy swftNessuna valutazione finora
- Thyroid Dysfunction and Reproductive Health: ReviewDocumento7 pagineThyroid Dysfunction and Reproductive Health: ReviewAnca CucuNessuna valutazione finora
- Diagnosis and Evaluation of Thyroid DisordersDocumento21 pagineDiagnosis and Evaluation of Thyroid DisordersIvan AditamaNessuna valutazione finora
- Thyroid Dalam KehamilanDocumento46 pagineThyroid Dalam KehamilanamriNessuna valutazione finora
- TIRMODDocumento66 pagineTIRMODYaniNessuna valutazione finora
- Drugstudy Revise Super FinallllllDocumento18 pagineDrugstudy Revise Super FinallllllLia DicksonNessuna valutazione finora
- Endocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Documento17 pagineEndocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Ali AlyahawiNessuna valutazione finora
- Thyroid GlandDocumento9 pagineThyroid GlandZach ReyesNessuna valutazione finora
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocumento71 pagineThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyNessuna valutazione finora
- Thyroid Function Tests and Goitre SV 24-4-21Documento51 pagineThyroid Function Tests and Goitre SV 24-4-21Lal KhanNessuna valutazione finora
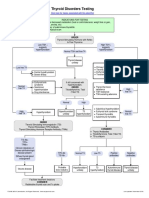
- Thyroid Disorders Testing AlgorithmDocumento1 paginaThyroid Disorders Testing AlgorithmkatNessuna valutazione finora
- Thyroid Gland: Anatomy, Physiology and Disease ManagementDocumento127 pagineThyroid Gland: Anatomy, Physiology and Disease ManagementCarla Mae MoraNessuna valutazione finora
- Thyroid Function, Levels and Disorders ExplainedDocumento46 pagineThyroid Function, Levels and Disorders ExplainedsinayupeNessuna valutazione finora
- Thyroid: Endocrine DiseaseDocumento20 pagineThyroid: Endocrine DiseasehoneymishraNessuna valutazione finora
- Clinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmDocumento73 pagineClinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmdiniNessuna valutazione finora
- Pharmacology Finals Lecture Thyroid DisordersDocumento11 paginePharmacology Finals Lecture Thyroid DisordersJuliann100% (1)
- Hypothyroid in Pregnancy Andi CakraDocumento32 pagineHypothyroid in Pregnancy Andi CakraCakraEkkyNessuna valutazione finora
- Thyroid Function Tests ExplainedDocumento25 pagineThyroid Function Tests ExplainedEva SinghNessuna valutazione finora
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocumento89 pagine4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- Endocrinology Part 2Documento4 pagineEndocrinology Part 2Alondra SagarioNessuna valutazione finora
- Thyroid Disorders Testing AlgorithmDocumento1 paginaThyroid Disorders Testing AlgorithmMuhamad SuriansyahNessuna valutazione finora
- Thyroid Testing AlgorithmDocumento1 paginaThyroid Testing AlgorithmRezi HelperNessuna valutazione finora
- NCM EndoDocumento23 pagineNCM EndoArriza Kryssan SoriaNessuna valutazione finora
- TOG Thyroid Dysfunction and Reproductive HealthDocumento7 pagineTOG Thyroid Dysfunction and Reproductive HealthMarNessuna valutazione finora
- Hipo AsrticulDocumento6 pagineHipo AsrticulKarol MurciaNessuna valutazione finora
- Disorders of Thyroid FunctionDocumento83 pagineDisorders of Thyroid FunctionSteven Andriie0% (1)
- Hyperthyroidism in PregnancyDocumento21 pagineHyperthyroidism in PregnancyCharisse Aser Flores AquinoNessuna valutazione finora
- Nodular Non Toxic GoiterDocumento36 pagineNodular Non Toxic Goiterjean_arellanoNessuna valutazione finora
- Hyperthyroid DisordersDocumento49 pagineHyperthyroid Disordersayu permata dewiNessuna valutazione finora
- Hashimoto's Thyroiditis InfographicDocumento2 pagineHashimoto's Thyroiditis InfographicPetraNessuna valutazione finora
- Thyroid DiseasesDocumento44 pagineThyroid DiseasesPLDT HOMENessuna valutazione finora
- Hypertiroidismo Review Lancet 2022Documento17 pagineHypertiroidismo Review Lancet 2022Diana Catalina Avila BareñoNessuna valutazione finora
- Disorders of the Thyroid: A Guide to Diagnosis and TreatmentDocumento36 pagineDisorders of the Thyroid: A Guide to Diagnosis and TreatmentMita Erna WatiNessuna valutazione finora
- Hypothyroidism: Hormones & YouDocumento1 paginaHypothyroidism: Hormones & YoufelminaNessuna valutazione finora
- HypothyroidismDocumento49 pagineHypothyroidismBahaa ShaabanNessuna valutazione finora
- Treatment of Hyperthyroidism: Western Medicine vs. Traditional Chinese MedicineDocumento6 pagineTreatment of Hyperthyroidism: Western Medicine vs. Traditional Chinese MedicineShahul HameedNessuna valutazione finora
- Persu Project FinalDocumento15 paginePersu Project FinalAshwinNessuna valutazione finora
- HIPERTIROIDDocumento30 pagineHIPERTIROIDNandaNessuna valutazione finora
- 6e - Thyroid Dysfunction in Pregnancy A Literature Review (Perbaiki Dafpus)Documento5 pagine6e - Thyroid Dysfunction in Pregnancy A Literature Review (Perbaiki Dafpus)KESEBELASAN RESOG 2023Nessuna valutazione finora
- Hiper Dan Hipotiroid (Revisi)Documento76 pagineHiper Dan Hipotiroid (Revisi)AgusNessuna valutazione finora
- Thyroid Talk-FMD RdsDocumento58 pagineThyroid Talk-FMD RdsSriman YarrarapuNessuna valutazione finora
- HYPOTHYROIDDocumento27 pagineHYPOTHYROIDTitin Tria UtamiNessuna valutazione finora
- Pi Is 2213858723000050Documento17 paginePi Is 2213858723000050lígia unievamedNessuna valutazione finora
- Thyroid PathophysiologyDocumento7 pagineThyroid PathophysiologyS RiarNessuna valutazione finora
- Thyroid: By: RickyDocumento116 pagineThyroid: By: Rickyricky hutagalungNessuna valutazione finora
- Thyroid Emergencies: The Art and Science of Infusion NursingDocumento6 pagineThyroid Emergencies: The Art and Science of Infusion NursingMohd Yanuar SaifudinNessuna valutazione finora
- FunctionTests BrochureDocumento2 pagineFunctionTests Brochurejonalyntonato09Nessuna valutazione finora
- Hashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandHashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Engineering Standards SAEC Waste Disposal LandfillsDocumento17 pagineEngineering Standards SAEC Waste Disposal LandfillsAhmad RazaNessuna valutazione finora
- MudreDocumento10 pagineMudrejezebelvertNessuna valutazione finora
- Role of Imaging in RhinologyDocumento223 pagineRole of Imaging in RhinologyDr. T. Balasubramanian100% (2)
- VITAMINS-Carol Jane Lorenzo, RMTDocumento8 pagineVITAMINS-Carol Jane Lorenzo, RMTREYES, JAN MERCK M.Nessuna valutazione finora
- Lung Cancer - Symptoms and Causes - Mayo ClinicDocumento9 pagineLung Cancer - Symptoms and Causes - Mayo ClinicTakuranashe DebweNessuna valutazione finora
- PH 021 enDocumento4 paginePH 021 enjohnllenalcantaraNessuna valutazione finora
- Wto Unit-2Documento19 pagineWto Unit-2Anwar KhanNessuna valutazione finora
- Soft Drinks in India: Euromonitor International February 2022Documento27 pagineSoft Drinks in India: Euromonitor International February 2022Gayathri22394Nessuna valutazione finora
- Dr. Abazar Habibinia's Guide to Overweight, Obesity, and Weight ManagementDocumento41 pagineDr. Abazar Habibinia's Guide to Overweight, Obesity, and Weight ManagementTasniiem KhmbataNessuna valutazione finora
- Chapter 22 The First Heart SoundDocumento5 pagineChapter 22 The First Heart SoundAbhilash ReddyNessuna valutazione finora
- Ijspt 10 734 PDFDocumento14 pagineIjspt 10 734 PDFasmaNessuna valutazione finora
- L Sit ProgramDocumento23 pagineL Sit Programdebo100% (1)
- Nursing Interventions for Ineffective Airway ClearanceDocumento3 pagineNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- PE GCSE Revision Quiz - Updated With AnswersDocumento40 paginePE GCSE Revision Quiz - Updated With AnswersmohitNessuna valutazione finora
- "PASS" Principles For Predictable PDFDocumento10 pagine"PASS" Principles For Predictable PDFkishan bordaNessuna valutazione finora
- MMI4804 Quiz 5Documento16 pagineMMI4804 Quiz 5Ham Mad0% (1)
- Environment in Palestine 1Documento28 pagineEnvironment in Palestine 1YOSEF DERDESAWENessuna valutazione finora
- Tradition With A Future: Solutions For Operative HysterosDocumento16 pagineTradition With A Future: Solutions For Operative Hysterosأحمد قائدNessuna valutazione finora
- Case Control Study For MedicDocumento41 pagineCase Control Study For Medicnunu ahmedNessuna valutazione finora
- Proximal Humerus Fractures Epidemiology and TrendsDocumento5 pagineProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesNessuna valutazione finora
- Weeblylp MedicinaDocumento18 pagineWeeblylp Medicinaapi-538325537Nessuna valutazione finora
- Lucas MattoonDocumento1 paginaLucas Mattoonapi-248178524Nessuna valutazione finora
- A. Define Infertility: Objectives: Intended Learning Outcomes That TheDocumento2 pagineA. Define Infertility: Objectives: Intended Learning Outcomes That TheJc Mae CuadrilleroNessuna valutazione finora
- 11 - Chapter 7 PDFDocumento41 pagine11 - Chapter 7 PDFRakesh RakiNessuna valutazione finora
- BDD Fact SheetDocumento2 pagineBDD Fact SheetKeen ZeahNessuna valutazione finora
- Facts of MaintenanceDocumento9 pagineFacts of Maintenancegeorge youssefNessuna valutazione finora
- Brand Analysis of Leading Sanitary Napkin BrandsDocumento21 pagineBrand Analysis of Leading Sanitary Napkin BrandsSoumya PattnaikNessuna valutazione finora
- Fitness WalkingDocumento60 pagineFitness WalkingJC LeriaNessuna valutazione finora
- Stressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDocumento22 pagineStressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDarleen Rizel CalumbaNessuna valutazione finora
- Legalizing abortion in the Philippines for women's health and rightsDocumento2 pagineLegalizing abortion in the Philippines for women's health and rightsRosario Antoniete R. Cabilin100% (1)