Potrebbero piacerti anche
- Cardiac Disease NotesDocumento4 pagineCardiac Disease NotesKyla Mae JumaritoNessuna valutazione finora
- Competency AppraisalDocumento43 pagineCompetency AppraisalErica Ruvie AgbayaniNessuna valutazione finora
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisDa EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisValutazione: 5 su 5 stelle5/5 (1)
- Cardiovascular System 1Documento21 pagineCardiovascular System 1Johnmer AvelinoNessuna valutazione finora
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtDa EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtValutazione: 5 su 5 stelle5/5 (1)
- Disease Signs and Symptoms Lab Findings Pathophysiology Nursing Interventions Drug Study/ NRSG ResponsibilitiesDocumento37 pagineDisease Signs and Symptoms Lab Findings Pathophysiology Nursing Interventions Drug Study/ NRSG ResponsibilitiesEmmanuel Valmonte100% (11)
- MSN - EndocarditisDocumento6 pagineMSN - EndocarditisDanica AluraBalguaNessuna valutazione finora
- Integrative Anatomy and Pathophysiology in TCM CardiologyDa EverandIntegrative Anatomy and Pathophysiology in TCM CardiologyNessuna valutazione finora
- CVS CaseDocumento10 pagineCVS Casedoctorumahoney777Nessuna valutazione finora
- Applied AnaphyDocumento22 pagineApplied AnaphypikaNessuna valutazione finora
- Ortho VIVA TopicsDocumento22 pagineOrtho VIVA TopicsSiti RaudahNessuna valutazione finora
- Critical Care ChallengesDocumento17 pagineCritical Care ChallengesYnaffit Alteza UntalNessuna valutazione finora
- MS Nursing ReviewerDocumento16 pagineMS Nursing ReviewerSunshine SiopaoNessuna valutazione finora
- 07 The Valvular PatientDocumento83 pagine07 The Valvular PatientDanielaNessuna valutazione finora
- Git SystemDocumento16 pagineGit SystemedithlucnasNessuna valutazione finora
- Coronary Artherosclerosis - ACS and MIDocumento5 pagineCoronary Artherosclerosis - ACS and MIAila HinlogNessuna valutazione finora
- CardioDocumento122 pagineCardioAdrian Rosell Carrillo EnriquezNessuna valutazione finora
- Congenital Heart DseDocumento14 pagineCongenital Heart DseJedzRNNessuna valutazione finora
- Cardiovascular System 3Documento28 pagineCardiovascular System 3Kris Adrian MallillinNessuna valutazione finora
- Ms Penta NotesDocumento84 pagineMs Penta Notesshenric16Nessuna valutazione finora
- Cardiovascular SystemDocumento10 pagineCardiovascular Systemtheglobalnursing75% (4)
- Medsurg PrintDocumento82 pagineMedsurg PrintjennywatsurproblemNessuna valutazione finora
- Head Injury TLSDocumento51 pagineHead Injury TLSNay SoeNessuna valutazione finora
- ABC Handouts Part 3Documento5 pagineABC Handouts Part 3Pagente, Sofia Lorrene W.Nessuna valutazione finora
- Medical and Surgical Nursing Notes For NLEDocumento63 pagineMedical and Surgical Nursing Notes For NLEBel Zeta DonaireNessuna valutazione finora
- Personal History: Notes in Clinical CardiologyDocumento19 paginePersonal History: Notes in Clinical CardiologyRachitha GuttaNessuna valutazione finora
- Medicine NeckDocumento102 pagineMedicine NeckMukesh KhatiNessuna valutazione finora
- MEdical Surgical REVEWERDocumento86 pagineMEdical Surgical REVEWERennaedNessuna valutazione finora
- Respi DisorderDocumento14 pagineRespi DisorderErika ArceoNessuna valutazione finora
- سريرية كمبيوتر-1Documento11 pagineسريرية كمبيوتر-1مخلب كونوهاNessuna valutazione finora
- Medical Surgical: Nervous SystemDocumento90 pagineMedical Surgical: Nervous SystemCatherine G. Borras100% (1)
- MS ReviewDocumento82 pagineMS ReviewRey P. Del RosarioNessuna valutazione finora
- MedicalSurgical Nursing ReviewDocumento89 pagineMedicalSurgical Nursing ReviewPopa D. SilviuNessuna valutazione finora
- 1cardiovascular System DisordersDocumento13 pagine1cardiovascular System DisordersArvin MalondrasNessuna valutazione finora
- Medical Surgical Nursing - Nervous System: CoverageDocumento10 pagineMedical Surgical Nursing - Nervous System: CoverageDianne TolentinoNessuna valutazione finora
- MedicalSurgical Nursing ReviewDocumento86 pagineMedicalSurgical Nursing ReviewPopa D. SilviuNessuna valutazione finora
- Medical Surgical: SNS (Anti-Cholinergic/adrenergic)Documento12 pagineMedical Surgical: SNS (Anti-Cholinergic/adrenergic)Pedro SorianoNessuna valutazione finora
- Endocrine ReviewerDocumento14 pagineEndocrine Revieweraberly25Nessuna valutazione finora
- سريرية كمبيوترDocumento11 pagineسريرية كمبيوترمخلب كونوهاNessuna valutazione finora
- E Learning PerlimDocumento24 pagineE Learning PerlimAhmad BaolayyanNessuna valutazione finora
- Notes For Responses To Altered Tissue PerfusionDocumento12 pagineNotes For Responses To Altered Tissue Perfusiondivine armentonNessuna valutazione finora
- Cardio PPT BasedDocumento17 pagineCardio PPT Basedgindie ceraNessuna valutazione finora
- Medical Surgical Nursing Outline B - Joshua DiaoDocumento17 pagineMedical Surgical Nursing Outline B - Joshua DiaoLevi Rae CLerigo EstiponaNessuna valutazione finora
- Veterinary Internal MedicineDocumento233 pagineVeterinary Internal MedicineSulove KoiralaNessuna valutazione finora
- Medical Surgical Reviewer: NorepinephrineDocumento12 pagineMedical Surgical Reviewer: Norepinephrineitsme_rizaNessuna valutazione finora
- Cardiovascular & Hematologic SystemDocumento163 pagineCardiovascular & Hematologic SystemRellie CastroNessuna valutazione finora
- MS Notes 1Documento75 pagineMS Notes 1Marygrace Gan SabanalNessuna valutazione finora
- CN 118 - Assessment (Reviewer)Documento5 pagineCN 118 - Assessment (Reviewer)Camille SanguyoNessuna valutazione finora
- Welcome: What We All Should KnowDocumento44 pagineWelcome: What We All Should KnowSuman ShahNessuna valutazione finora
- Handouts Cardio RespiDocumento8 pagineHandouts Cardio Respijon elleNessuna valutazione finora
- Neonatal AsphyxiaDocumento35 pagineNeonatal AsphyxiaAsha jilu67% (3)
- Acute Coronary Syndrome: Kingdom of Saudi Arabia Ministry of Health King Fahad Hofuf Hospital Nursing EducationDocumento33 pagineAcute Coronary Syndrome: Kingdom of Saudi Arabia Ministry of Health King Fahad Hofuf Hospital Nursing EducationAqeelNessuna valutazione finora
- Medsurg ReviewerDocumento9 pagineMedsurg ReviewerAmirrah LaurenteNessuna valutazione finora
- Medical Surgical: Nervous SystemDocumento94 pagineMedical Surgical: Nervous SystemAngelika DomondonNessuna valutazione finora
- Inflamasi Perikardium: Pada Lapisan Jantung Lapisan Luar & Dalam Acute Atau ChronicDocumento17 pagineInflamasi Perikardium: Pada Lapisan Jantung Lapisan Luar & Dalam Acute Atau ChronicAi MioNessuna valutazione finora
- Grand Osce ReviewerDocumento16 pagineGrand Osce ReviewerBA Ong100% (1)
- Medicine Test On CVS Respiratory EndocrinologyDocumento10 pagineMedicine Test On CVS Respiratory EndocrinologyNavid BabluNessuna valutazione finora
- Lacerated WoundDocumento38 pagineLacerated Wounddomzlr18100% (2)
- Instructors GuideDocumento1 paginaInstructors Guidedomzlr18Nessuna valutazione finora
- BLEEDINGDocumento3 pagineBLEEDINGdomzlr18Nessuna valutazione finora
- Myocardial InfarctionDocumento1 paginaMyocardial Infarctiondomzlr18Nessuna valutazione finora
- THESIS APA FormatDocumento4 pagineTHESIS APA Formatdomzlr18100% (1)
- X3 SN DR13WNSDocumento1 paginaX3 SN DR13WNSdomzlr18Nessuna valutazione finora
- PregnancyDocumento1 paginaPregnancydomzlr18Nessuna valutazione finora
- Calendario LakersDocumento1 paginaCalendario LakersLorenzo GenovesiNessuna valutazione finora
- 2ENGLISH10 - Q1 - Module 2 - Week2 - Determine The Effect of Textual Aids On Understanding A Text - v4BDocumento25 pagine2ENGLISH10 - Q1 - Module 2 - Week2 - Determine The Effect of Textual Aids On Understanding A Text - v4Bcodm PlayerNessuna valutazione finora
- Admission, Criteria - Adult Intensive Care Unit.Documento5 pagineAdmission, Criteria - Adult Intensive Care Unit.EsamNessuna valutazione finora
- CV By, Yvette02Documento4 pagineCV By, Yvette02Yvette PamatmatNessuna valutazione finora
- Clinical Pathway TB Org AnakDocumento2 pagineClinical Pathway TB Org AnakRengganis PutriNessuna valutazione finora
- Seidman 2014Documento17 pagineSeidman 2014Anonymous G6zDTD2yNessuna valutazione finora
- JMO Handbook Updated 05 04 21 by Kate CushDocumento31 pagineJMO Handbook Updated 05 04 21 by Kate CushCrystal ZawNessuna valutazione finora
- GloukomaDocumento7 pagineGloukomaGraitaaNessuna valutazione finora
- Anaphylaxis Guidelines PosterDocumento1 paginaAnaphylaxis Guidelines PosterBabo SanNessuna valutazione finora
- Diare Akut: Adhesi Invasi Sitotoksin EnterotoksinDocumento4 pagineDiare Akut: Adhesi Invasi Sitotoksin EnterotoksinVeronica Yosita AnandaNessuna valutazione finora
- Etiology and Pathophysiology of Pleural EffusionDocumento17 pagineEtiology and Pathophysiology of Pleural EffusionFelix Wafula MusibiNessuna valutazione finora
- 2016 CIS Annual Meeting Immune Deficiency & DysregulationDocumento100 pagine2016 CIS Annual Meeting Immune Deficiency & DysregulationMetallum MarionetteNessuna valutazione finora
- A Systematic Review On Shifting Trends of Foodborne Diseases in PakistanDocumento16 pagineA Systematic Review On Shifting Trends of Foodborne Diseases in PakistanAbasyn Journal of Life SciencesNessuna valutazione finora
- EW Cordingley - Principles and Practice of NaturopathyDocumento28 pagineEW Cordingley - Principles and Practice of NaturopathyMitchellSNessuna valutazione finora
- Pgi Physiology Exam: Your Email AddressDocumento1 paginaPgi Physiology Exam: Your Email AddressCharlie65129Nessuna valutazione finora
- Contemporary Psychiatric-Mental Health Nursing 3rd Edition Kneisl Solutions Manual DownloadDocumento9 pagineContemporary Psychiatric-Mental Health Nursing 3rd Edition Kneisl Solutions Manual DownloadClarence Steele100% (24)
- English Assignments About Case Study Name: Indriyani Eka Lani Oematan NIM: 01.2.17.00609Documento4 pagineEnglish Assignments About Case Study Name: Indriyani Eka Lani Oematan NIM: 01.2.17.00609Eka OematanNessuna valutazione finora
- Loneliness and Mental Health: Chris BarberDocumento6 pagineLoneliness and Mental Health: Chris BarberHà Anh Lê VũNessuna valutazione finora
- 2 IrritableBowelSyndromeDocumento10 pagine2 IrritableBowelSyndromeRana EL-BakryNessuna valutazione finora
- Glaucoma: AetiologyDocumento3 pagineGlaucoma: Aetiologyjames cordenNessuna valutazione finora
- Review Unit 2Documento11 pagineReview Unit 2minyoongiNessuna valutazione finora
- Dental Management of Patients With CHFDocumento4 pagineDental Management of Patients With CHFarjayNessuna valutazione finora
- Homotoxicology 6 Phase TableDocumento1 paginaHomotoxicology 6 Phase TableSamNessuna valutazione finora
- Bowel ObstructionDocumento48 pagineBowel ObstructionPatrick John100% (1)
- лекц10Documento41 pagineлекц10A A D H INessuna valutazione finora
- Food Security: Its Components and ChallengesDocumento9 pagineFood Security: Its Components and ChallengesSimlindile NgobelaNessuna valutazione finora
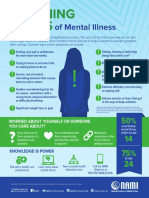
- Warning Signs of Mental IllnessDocumento1 paginaWarning Signs of Mental IllnessKierstenNessuna valutazione finora
- The Severe and Persistent Mental Illness Treatment Planner Practiceplanners Ebook PDF VersionDocumento58 pagineThe Severe and Persistent Mental Illness Treatment Planner Practiceplanners Ebook PDF Versionpaul.trivino34896% (27)
- IMAGINE+Caregiver+Program SSA+Documento59 pagineIMAGINE+Caregiver+Program SSA+Nikola VeleskiNessuna valutazione finora
- Lai, M.-C., & Baron-Cohen, S. (2015) - Identifying The Lost Generation of Adults With Autism Spectrum ConditionsDocumento15 pagineLai, M.-C., & Baron-Cohen, S. (2015) - Identifying The Lost Generation of Adults With Autism Spectrum ConditionsTomislav Cvrtnjak100% (1)
- Advanced DirectivesDocumento5 pagineAdvanced DirectivesJasmine CorreosNessuna valutazione finora