Potrebbero piacerti anche
- Direct Control of The Retinal FieldDocumento5 pagineDirect Control of The Retinal FieldneuroneuroNessuna valutazione finora
- Incredible Analysis GannDocumento5 pagineIncredible Analysis Gannpaparock34Nessuna valutazione finora
- Direct Control of The 'Retinal Field': Report On Three CasesDocumento11 pagineDirect Control of The 'Retinal Field': Report On Three CasesneuroneuroNessuna valutazione finora
- Spectrum CurrentDocumento1 paginaSpectrum CurrentXmd InOutNessuna valutazione finora
- WECOC - Diagnosing HypertensionDocumento37 pagineWECOC - Diagnosing HypertensionDhira 'Princess Kalonk' AninditaNessuna valutazione finora
- Place, U.T. - Is Consciousness A Brain ProcessDocumento6 paginePlace, U.T. - Is Consciousness A Brain Processgalen_mitchellNessuna valutazione finora
- Guillain Barre SyndromeDocumento170 pagineGuillain Barre SyndromeAfra HanifiNessuna valutazione finora
- Sungod The Most Probable Theory of Our TimeDocumento68 pagineSungod The Most Probable Theory of Our Timeanon-386572Nessuna valutazione finora
- Geometry: Lines and AnglesDocumento19 pagineGeometry: Lines and AnglesOm ShrikantNessuna valutazione finora
- RSI ResidentDocumento58 pagineRSI ResidentHidayati IdaNessuna valutazione finora
- W. D. Gann: The Basis of My Forecasting MethodDocumento12 pagineW. D. Gann: The Basis of My Forecasting MethodwupuweiNessuna valutazione finora
- Sub Sci Master Key SystemDocumento157 pagineSub Sci Master Key SystemjagyoujealoousNessuna valutazione finora
- 3730 Monitoring Hemodinamik-2019Documento52 pagine3730 Monitoring Hemodinamik-2019ojika olandaNessuna valutazione finora
- Their Hearts Were Hardened John L. McLaughlinDocumento26 pagineTheir Hearts Were Hardened John L. McLaughlinHumayun Sunil100% (1)
- Solar Fire Interpretations Report Standard Natal InterpretationsDocumento17 pagineSolar Fire Interpretations Report Standard Natal InterpretationsAnand Chiney100% (1)
- Traditional Chinese MedicineDocumento4 pagineTraditional Chinese MedicinekmlNessuna valutazione finora
- How To Measure BPDocumento25 pagineHow To Measure BPSenen PaezNessuna valutazione finora
- Icare BookDocumento20 pagineIcare Booknithin100% (1)
- How To Trade in Stocks 2 of 2Documento8 pagineHow To Trade in Stocks 2 of 2James RiceNessuna valutazione finora
- Studentsassistan00hack PDFDocumento196 pagineStudentsassistan00hack PDFjonn1eNessuna valutazione finora
- Ter at OlogyDocumento23 pagineTer at OlogyRana VandanaNessuna valutazione finora
- Hursts Eight Principals of Cycle AnalysisDocumento1 paginaHursts Eight Principals of Cycle AnalysisVijay VijiNessuna valutazione finora
- Customized Geometric Risk Premium EstimatorDocumento41 pagineCustomized Geometric Risk Premium EstimatorCardoso PenhaNessuna valutazione finora
- CPR - Cardiopulmonary ResuscitationDocumento31 pagineCPR - Cardiopulmonary ResuscitationPanji HerlambangNessuna valutazione finora
- 40-Year Cycle:: Stocks in 2018 - 2021 VIDocumento6 pagine40-Year Cycle:: Stocks in 2018 - 2021 VIturtlespiritflutesNessuna valutazione finora
- HistogramDocumento17 pagineHistogramsaifieNessuna valutazione finora
- Math in Finance MITDocumento22 pagineMath in Finance MITkkappaNessuna valutazione finora
- D Gann Research Paper THEO530Documento16 pagineD Gann Research Paper THEO530dkgannNessuna valutazione finora
- Flanagan Webinar SlidesDocumento36 pagineFlanagan Webinar SlidesOshawawookiesNessuna valutazione finora
- Interpretation of Stress TestsDocumento26 pagineInterpretation of Stress TestsHashini VjkmrNessuna valutazione finora
- Gurdjieff - Paul Van Oyen - The - Enneagram - Now - 1 - 2 - 3Documento24 pagineGurdjieff - Paul Van Oyen - The - Enneagram - Now - 1 - 2 - 3enrick71Nessuna valutazione finora
- Intubation ProcedureDocumento5 pagineIntubation ProcedurePurwadi SujalmoNessuna valutazione finora
- Hemodynamic MonitoringDocumento3 pagineHemodynamic MonitoringNadiah IsmailNessuna valutazione finora
- Astro Econ Monthly InfoDocumento5 pagineAstro Econ Monthly InfoloshudeNessuna valutazione finora
- Green, Dave - Gann Angles and SquaresDocumento4 pagineGreen, Dave - Gann Angles and SquaresscooexNessuna valutazione finora
- Name: Dr. Saroj Kumar Lenka Date of Birth: Present AddressDocumento10 pagineName: Dr. Saroj Kumar Lenka Date of Birth: Present Addressanon-147048100% (2)
- PR 127782Documento4 paginePR 127782kaiowas886Nessuna valutazione finora
- The Sacred Versus The Secular: Nasr On Science: Vincit Omnia Veritas. III, 1Documento19 pagineThe Sacred Versus The Secular: Nasr On Science: Vincit Omnia Veritas. III, 1oceanmist0101Nessuna valutazione finora
- Recommendations For Sepsis Management in Limited SourcesDocumento25 pagineRecommendations For Sepsis Management in Limited SourcesFatahillah NazarNessuna valutazione finora
- Future CyclesDocumento4 pagineFuture CyclesbrahimNessuna valutazione finora
- Measurement ScaleDocumento223 pagineMeasurement ScaleBiswaranjan JenaNessuna valutazione finora
- Kaldor - 1939 - Speculation and Economic StabilityDocumento28 pagineKaldor - 1939 - Speculation and Economic Stabilityjpkoning100% (1)
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDocumento52 pagineSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNessuna valutazione finora
- Jeremy Miles, Mark Shevlin Applying Regression and CorrelationDocumento230 pagineJeremy Miles, Mark Shevlin Applying Regression and CorrelationMarKo TonČićNessuna valutazione finora
- Song For CatherineDocumento2 pagineSong For CatherineJustin PyneNessuna valutazione finora
- Ehlers. The CG OscillatorDocumento4 pagineEhlers. The CG OscillatorPapy RysNessuna valutazione finora
- 142FFTDocumento4 pagine142FFTEduardo FerreiraNessuna valutazione finora
- Ogdensburg Journal 1909 January JuneDocumento1 paginaOgdensburg Journal 1909 January Junepgeronazzo8450Nessuna valutazione finora
- Harvard IRIDocumento39 pagineHarvard IRIBarry100% (1)
- Aether Analytics Technical Conspectus July 11, 2014Documento54 pagineAether Analytics Technical Conspectus July 11, 2014Alex Bernal, CMT100% (1)
- Trade CyclesDocumento10 pagineTrade CyclessushmasomannaNessuna valutazione finora
- Basics of VentilationDocumento69 pagineBasics of Ventilationdr_nkhan3415Nessuna valutazione finora
- 01 CycleOfGrowth PricesDocumento1 pagina01 CycleOfGrowth Pricesnikesh_prasadNessuna valutazione finora
- Delta NotesDocumento1 paginaDelta NotesJack GannNessuna valutazione finora
- Planet - : EconomicsDocumento9 paginePlanet - : EconomicsVenkatNessuna valutazione finora
- Cardiopulmonary ResuscitationDocumento38 pagineCardiopulmonary ResuscitationAgus SyaifudinNessuna valutazione finora
- Basic Life Support For Healthcare Providers (BLS) : Presented By: Youssef Youssef RT Respiratory Therapy DepartementDocumento43 pagineBasic Life Support For Healthcare Providers (BLS) : Presented By: Youssef Youssef RT Respiratory Therapy Departementkurt94764Nessuna valutazione finora
- Patient CareDocumento20 paginePatient CareVincent QuitorianoNessuna valutazione finora
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDa EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesValutazione: 5 su 5 stelle5/5 (2)
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocumento112 pagineClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNessuna valutazione finora
- Pain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityDocumento11 paginePain Scale and Its Types: Quratulain Mughal Batch Iv Doctor of Physical Therapy Isra UniversityNilakshi Barik MandalNessuna valutazione finora
- Birth Injuries in Neonates: Pediatrics in Review November 2016Documento15 pagineBirth Injuries in Neonates: Pediatrics in Review November 2016Nilakshi Barik MandalNessuna valutazione finora
- Pain AssessmentDocumento12 paginePain AssessmentFadhilah Asyifa DewantiNessuna valutazione finora
- Examination of The Breast: 11/14/2011 © Clinical Skills Resource Centre, University of Liverpool, UKDocumento19 pagineExamination of The Breast: 11/14/2011 © Clinical Skills Resource Centre, University of Liverpool, UKNilakshi Barik MandalNessuna valutazione finora
- Mentalhealthactppt 160524140542Documento34 pagineMentalhealthactppt 160524140542Nilakshi Barik MandalNessuna valutazione finora
- Implanon: Subdermal Single Rod Contraceptive ImplantDocumento4 pagineImplanon: Subdermal Single Rod Contraceptive ImplantNilakshi Barik MandalNessuna valutazione finora
- New Format With Correct LayoutDocumento3 pagineNew Format With Correct LayoutNilakshi Barik MandalNessuna valutazione finora
- Pptforphysical 130322221925 Phpapp01Documento117 paginePptforphysical 130322221925 Phpapp01Karen Mae Santiago AlcantaraNessuna valutazione finora
- Physical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NDocumento41 paginePhysical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NNilakshi Barik MandalNessuna valutazione finora
- Presented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowDocumento93 paginePresented By: Sandeep Yadav M.Sc. (N) 1 Year KGMU LucknowNilakshi Barik MandalNessuna valutazione finora
- PreconceptionDocumento29 paginePreconceptionNilakshi Barik MandalNessuna valutazione finora
- History and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyDocumento84 pagineHistory and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyNilakshi Barik MandalNessuna valutazione finora
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocumento112 pagineClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNessuna valutazione finora
- Oral Hygiene: Mrs - NilakshiDocumento11 pagineOral Hygiene: Mrs - NilakshiNilakshi Barik MandalNessuna valutazione finora
- Ijshr0038 PDFDocumento9 pagineIjshr0038 PDFNilakshi Barik MandalNessuna valutazione finora
- Monica Rita Hendricks PDFDocumento151 pagineMonica Rita Hendricks PDFNilakshi Barik MandalNessuna valutazione finora
- Pain Manage Me NT: Ms - Nilakshi Barik MandalDocumento14 paginePain Manage Me NT: Ms - Nilakshi Barik MandalNilakshi Barik MandalNessuna valutazione finora
- Ms. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesDocumento11 pagineMs. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesNilakshi Barik MandalNessuna valutazione finora
- Gate Control TheoryDocumento6 pagineGate Control TheoryNilakshi Barik MandalNessuna valutazione finora
- Gate Contro L Theory: Ms - Nilakshi Barik MandalDocumento6 pagineGate Contro L Theory: Ms - Nilakshi Barik MandalNilakshi Barik MandalNessuna valutazione finora
- Ms. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesDocumento11 pagineMs. Nilakshi Barik Mandal Lecturer Oxford College of Nursing SciencesNilakshi Barik MandalNessuna valutazione finora
- History and Physical Assessment of Integumentary System: Mrs - Nilakshi Barik LecturerDocumento84 pagineHistory and Physical Assessment of Integumentary System: Mrs - Nilakshi Barik LecturerNilakshi Barik MandalNessuna valutazione finora
- Medical Surgical Nursing AssignmentDocumento166 pagineMedical Surgical Nursing AssignmentSonali Sengar0% (1)
- Preconception CouncellDocumento48 paginePreconception CouncellNilakshi Barik MandalNessuna valutazione finora
- Fetal SkullDocumento5 pagineFetal SkullNilakshi Barik MandalNessuna valutazione finora
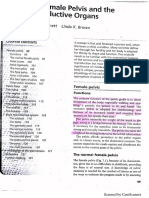
- Female PelvisDocumento7 pagineFemale PelvisNilakshi Barik MandalNessuna valutazione finora
- Unit Plan For I Year BSC Nursing NUTRITION BATCH 2019-2020: Total Hours:60 HrsDocumento1 paginaUnit Plan For I Year BSC Nursing NUTRITION BATCH 2019-2020: Total Hours:60 HrsNilakshi Barik MandalNessuna valutazione finora
- Nutrition Course PlanDocumento7 pagineNutrition Course PlanNilakshi Barik MandalNessuna valutazione finora
- Checklist of Quality Indicators For NABH Accreditation PreparationDocumento11 pagineChecklist of Quality Indicators For NABH Accreditation PreparationQUALITY SIDARTH HOSPITALSNessuna valutazione finora
- Actinic KeratosisDocumento19 pagineActinic KeratosisDajour CollinsNessuna valutazione finora
- Senior CapstoneDocumento6 pagineSenior Capstoneapi-313278667Nessuna valutazione finora
- FREE PRINTABLE CNA Practice ExamDocumento12 pagineFREE PRINTABLE CNA Practice Examheartandhandstraining_com91% (57)
- Legal Medicine: Legal Medicine (2011) Antonio Rebosa, LL.B, M.DDocumento6 pagineLegal Medicine: Legal Medicine (2011) Antonio Rebosa, LL.B, M.DarciblueNessuna valutazione finora
- Obgyn Physician Assistant 1Documento3 pagineObgyn Physician Assistant 1api-558916281Nessuna valutazione finora
- Frequency of Depression, Anxiety and Stress in Patients Referred For Endoscopy With Symptoms of DyspepsiaDocumento5 pagineFrequency of Depression, Anxiety and Stress in Patients Referred For Endoscopy With Symptoms of DyspepsiaSana SajidNessuna valutazione finora
- Patient Record BookDocumento1 paginaPatient Record BooksumarumNessuna valutazione finora
- Acute Cholecystitis: Jochen Schuld Matthias GlanemannDocumento3 pagineAcute Cholecystitis: Jochen Schuld Matthias GlanemannNabilla DamarNessuna valutazione finora
- DementiaDocumento26 pagineDementianadya100% (4)
- Antenatal Care: Muhammad Wasil Khan and Ramsha MazharDocumento55 pagineAntenatal Care: Muhammad Wasil Khan and Ramsha MazharmarviNessuna valutazione finora
- 3in1 Shoulder BlockDocumento2 pagine3in1 Shoulder BlockTejasvi ChandranNessuna valutazione finora
- 2019 Dent4060Documento10 pagine2019 Dent4060Jason JNessuna valutazione finora
- Danish Mask StudyDocumento1 paginaDanish Mask StudyJuana AtkinsNessuna valutazione finora
- Bell 2015Documento5 pagineBell 2015Afien MuktiNessuna valutazione finora
- News Story 3Documento2 pagineNews Story 3api-558280939Nessuna valutazione finora
- DR - Neimy Novitasari. SpsDocumento56 pagineDR - Neimy Novitasari. Spscindy ramadhaniNessuna valutazione finora
- Important Causes of Sudden Cardiac DeathDocumento2 pagineImportant Causes of Sudden Cardiac DeathTausif AbbasNessuna valutazione finora
- ApheresisDocumento5 pagineApheresisGRK BIOMEDNessuna valutazione finora
- Adverse Drug ReactionDocumento15 pagineAdverse Drug ReactionPuji Arifianti RamadhanyNessuna valutazione finora
- Pga R3Documento71 paginePga R3Samruddhi PataitNessuna valutazione finora
- MPC-CPN Basics of Toxicology-HDocumento12 pagineMPC-CPN Basics of Toxicology-HNahid ParveenNessuna valutazione finora
- Saunders, Et Al (2017)Documento9 pagineSaunders, Et Al (2017)uki arrownaraNessuna valutazione finora
- Case Study Severe Depression With Psychosis.: Submitted To:-Submitted ByDocumento33 pagineCase Study Severe Depression With Psychosis.: Submitted To:-Submitted ByPallavi KharadeNessuna valutazione finora
- Aparat Elect Rot Era Pie Aries MDocumento2 pagineAparat Elect Rot Era Pie Aries MSorin NechiforNessuna valutazione finora
- Efficacy of Toltrazuril As A Metaphylactic and Therapeutic Treatment of Coccidiosis in First-Year Grazing CalvesDocumento8 pagineEfficacy of Toltrazuril As A Metaphylactic and Therapeutic Treatment of Coccidiosis in First-Year Grazing Calvesthanh ba matNessuna valutazione finora
- Borda2018 PDFDocumento48 pagineBorda2018 PDFlarasNessuna valutazione finora
- 811 2Documento16 pagine811 2almightyx10Nessuna valutazione finora
- The Little Book of Pediatrics PDFDocumento208 pagineThe Little Book of Pediatrics PDFPaulo GouveiaNessuna valutazione finora
- Animal Care QP U1Documento12 pagineAnimal Care QP U1boho14Nessuna valutazione finora