Potrebbero piacerti anche
- Air Pollution, Climate, and Health: An Integrated Perspective on Their InteractionsDa EverandAir Pollution, Climate, and Health: An Integrated Perspective on Their InteractionsMeng GaoNessuna valutazione finora
- Acp 2021 581Documento134 pagineAcp 2021 581Amaechi InnocentNessuna valutazione finora
- Environmental Resilience and Transformation in times of COVID-19: Climate Change Effects on Environmental FunctionalityDa EverandEnvironmental Resilience and Transformation in times of COVID-19: Climate Change Effects on Environmental FunctionalityA.L. RamanathanNessuna valutazione finora
- Key Questions in Environmental Toxicology: A Study and Revision GuideDa EverandKey Questions in Environmental Toxicology: A Study and Revision GuideNessuna valutazione finora
- COVID-19 in the Environment: Impact, Concerns, and Management of CoronavirusDa EverandCOVID-19 in the Environment: Impact, Concerns, and Management of CoronavirusNessuna valutazione finora
- Mitigation and Adaptation of Urban Overheating: The Impact of Warmer Cities on Climate, Energy, Health, Environmental Quality, Economy, and Quality of LifeDa EverandMitigation and Adaptation of Urban Overheating: The Impact of Warmer Cities on Climate, Energy, Health, Environmental Quality, Economy, and Quality of LifeNasrin AghamohammadiNessuna valutazione finora
- Adverse Effects of Engineered Nanomaterials: Exposure, Toxicology, and Impact on Human HealthDa EverandAdverse Effects of Engineered Nanomaterials: Exposure, Toxicology, and Impact on Human HealthBengt FadeelValutazione: 4 su 5 stelle4/5 (1)
- Portable Arduino Based Air Quality Monitoring System: Polytechnic University of The PhilippinesDocumento52 paginePortable Arduino Based Air Quality Monitoring System: Polytechnic University of The PhilippinesJerome BalatbatNessuna valutazione finora
- Chinnaswamy Et Al Association Between Outdoor Air Pollution and Cardiovascular Mortality in Bangalore 2013Documento7 pagineChinnaswamy Et Al Association Between Outdoor Air Pollution and Cardiovascular Mortality in Bangalore 2013shamalaksNessuna valutazione finora
- Essd 15 2295 2023Documento33 pagineEssd 15 2295 2023terezamlazaroNessuna valutazione finora
- Phe Final ReportDocumento26 paginePhe Final ReportPrathmesh Anil kadamNessuna valutazione finora
- HPH-18706 LancetLessons HealthyBuildings HighRes-2Documento7 pagineHPH-18706 LancetLessons HealthyBuildings HighRes-2LucasKaaioNessuna valutazione finora
- Assessing Progress Towards Sustainability: Frameworks, Tools and Case StudiesDa EverandAssessing Progress Towards Sustainability: Frameworks, Tools and Case StudiesCarmen TeodosiuNessuna valutazione finora
- Underground Sensing: Monitoring and Hazard Detection for Environment and InfrastructureDa EverandUnderground Sensing: Monitoring and Hazard Detection for Environment and InfrastructureSibel PamukcuNessuna valutazione finora
- Environmental Management of Waste Electrical and Electronic EquipmentDa EverandEnvironmental Management of Waste Electrical and Electronic EquipmentNessuna valutazione finora
- The UNEP-SETAC Toxicity Model: RecommendedDocumento15 pagineThe UNEP-SETAC Toxicity Model: RecommendedMichelle Quilaqueo NovoaNessuna valutazione finora
- Emerging Aquatic Contaminants: One Health Framework for Risk Assessment and Remediation in the Post COVID-19 AnthropoceneDa EverandEmerging Aquatic Contaminants: One Health Framework for Risk Assessment and Remediation in the Post COVID-19 AnthropoceneNessuna valutazione finora
- Sensors: Early Warning Systems For Covid-19 Infections Based On Low-Cost Indoor Air-Quality Sensors and LpwansDocumento23 pagineSensors: Early Warning Systems For Covid-19 Infections Based On Low-Cost Indoor Air-Quality Sensors and LpwansThomas TanNessuna valutazione finora
- Evaluating Viral Filtration Efficiency in Non-Centralized Air-Conditioning Systems A Novel Approach Grounded in Medical Experimental DataDocumento23 pagineEvaluating Viral Filtration Efficiency in Non-Centralized Air-Conditioning Systems A Novel Approach Grounded in Medical Experimental Dataraj cyberboyNessuna valutazione finora
- Environmental Aspects of Construction with Waste MaterialsDa EverandEnvironmental Aspects of Construction with Waste MaterialsNessuna valutazione finora
- The Microbiology of Nuclear Waste DisposalDa EverandThe Microbiology of Nuclear Waste DisposalJonathan R. LloydNessuna valutazione finora
- PHD Thesis On Air PollutionDocumento7 paginePHD Thesis On Air PollutionKayla Jones100% (2)
- Smart Nanomaterials to Combat the Spread of Viral Infections: Advanced Strategies for the Prevention of Viral InfectionsDa EverandSmart Nanomaterials to Combat the Spread of Viral Infections: Advanced Strategies for the Prevention of Viral InfectionsRaju KhanNessuna valutazione finora
- Environment and Development: Basic Principles, Human Activities, and Environmental ImplicationsDa EverandEnvironment and Development: Basic Principles, Human Activities, and Environmental ImplicationsValutazione: 5 su 5 stelle5/5 (1)
- Climate Extremes and Their Implications for Impact and Risk AssessmentDa EverandClimate Extremes and Their Implications for Impact and Risk AssessmentJana SillmannNessuna valutazione finora
- Adapting to Climate Change in Europe: Exploring Sustainable Pathways - From Local Measures to Wider PoliciesDa EverandAdapting to Climate Change in Europe: Exploring Sustainable Pathways - From Local Measures to Wider PoliciesHans SandersonNessuna valutazione finora
- COVID-19: Tackling Global Pandemics through Scientific and Social ToolsDa EverandCOVID-19: Tackling Global Pandemics through Scientific and Social ToolsS. ChatterjeeNessuna valutazione finora
- FILTRADocumento25 pagineFILTRADOUNIA BELLACHENessuna valutazione finora
- Characterization and Control of Odours and VOC in the Process IndustriesDa EverandCharacterization and Control of Odours and VOC in the Process IndustriesNessuna valutazione finora
- Environmental MicropollutantsDa EverandEnvironmental MicropollutantsMuhammad Zaffar HashmiNessuna valutazione finora
- Carbon Dioxide Utilisation: Closing the Carbon CycleDa EverandCarbon Dioxide Utilisation: Closing the Carbon CycleNessuna valutazione finora
- Journal of Electronic & Information Systems - Vol.5, Iss.1 October 2023Documento71 pagineJournal of Electronic & Information Systems - Vol.5, Iss.1 October 2023Bilingual PublishingNessuna valutazione finora
- Evaluating The Toxicity of Airborne Particulate Matter and Nanoparticles by Measuring Oxidative Stress Potential A Workshop Report and ConsensusDocumento26 pagineEvaluating The Toxicity of Airborne Particulate Matter and Nanoparticles by Measuring Oxidative Stress Potential A Workshop Report and ConsensusJota Gomez CdlmNessuna valutazione finora
- Global Trends in Biodiversity and Ecosystem ServicDocumento15 pagineGlobal Trends in Biodiversity and Ecosystem Servickenenisa.abdisastatNessuna valutazione finora
- IMPACT World+: A Globally Regionalized Life Cycle Impact Assessment MethodDocumento22 pagineIMPACT World+: A Globally Regionalized Life Cycle Impact Assessment MethodMSNessuna valutazione finora
- DENTENER - N and S Deposition Global Scales - 2006Documento21 pagineDENTENER - N and S Deposition Global Scales - 2006Anderson SantiNessuna valutazione finora
- Accepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Documento9 pagineAccepted Manuscript: It Is Time To Address Airborne Transmission of COVID-19Anonymous 9wHscMNessuna valutazione finora
- Natural Ventilation Characterization in A Classroom Under DifferentDocumento13 pagineNatural Ventilation Characterization in A Classroom Under DifferentconruyNessuna valutazione finora
- Module5 IMPACTS AirQualityManagementDocumento46 pagineModule5 IMPACTS AirQualityManagementFarhan WibiandraNessuna valutazione finora
- 3110007Documento3 pagine3110007Manvendra RaiNessuna valutazione finora
- Unani MedicineDocumento33 pagineUnani MedicineMalik Rizwan Elahi83% (6)
- Is US Health Really Best in The World PDFDocumento3 pagineIs US Health Really Best in The World PDFpartha9sarathi9ainNessuna valutazione finora
- L4 Motion - G9Documento24 pagineL4 Motion - G9Naresh world SinghNessuna valutazione finora
- PE ABH Why Should I Limit Sodium UCM - 300625 PDFDocumento2 paginePE ABH Why Should I Limit Sodium UCM - 300625 PDFClau E. de GregorioNessuna valutazione finora
- Is It The End of Modern Medicine?Documento2 pagineIs It The End of Modern Medicine?Garv JainNessuna valutazione finora
- Basic Body MassageDocumento4 pagineBasic Body MassageNaresh world SinghNessuna valutazione finora
- Ecemr 04 00114Documento3 pagineEcemr 04 00114PRAMIT KUMAR SENAPATINessuna valutazione finora
- BDocumento3 pagineBNaresh world SinghNessuna valutazione finora
- Exercises: Answer 1Documento3 pagineExercises: Answer 1Naresh world SinghNessuna valutazione finora
- © Ncert Not To Be Republished: Acids, Bases and SaltsDocumento9 pagine© Ncert Not To Be Republished: Acids, Bases and SaltsNaresh world SinghNessuna valutazione finora
- ValenceDocumento1 paginaValenceMisbah PatelNessuna valutazione finora
- Definition of Science From RMDocumento22 pagineDefinition of Science From RMMargusWaffaNessuna valutazione finora
- 3224 Topper 21 110 1 2 392 1102 Basics of Chemistry Up201508251715 14405031Documento9 pagine3224 Topper 21 110 1 2 392 1102 Basics of Chemistry Up201508251715 14405031Naresh world SinghNessuna valutazione finora
- Jeep 103Documento10 pagineJeep 103mohapatramugdha99Nessuna valutazione finora
- CDocumento4 pagineCNaresh world SinghNessuna valutazione finora
- Learn CBSE: Body Movements Class 6 Extra Questions Science Chapter 8Documento5 pagineLearn CBSE: Body Movements Class 6 Extra Questions Science Chapter 8Naresh world SinghNessuna valutazione finora
- Learn CBSE: Body Movements Class 6 Extra Questions Science Chapter 8Documento3 pagineLearn CBSE: Body Movements Class 6 Extra Questions Science Chapter 8Naresh world SinghNessuna valutazione finora
- Respiratory Virus Infections: Understanding COVID-19: PrimerDocumento5 pagineRespiratory Virus Infections: Understanding COVID-19: PrimerNaresh world SinghNessuna valutazione finora
- Outcomes of Hydroxychloroquine Usage in United States Veterans Hospitalized With Covid-19Documento27 pagineOutcomes of Hydroxychloroquine Usage in United States Veterans Hospitalized With Covid-19Naresh world SinghNessuna valutazione finora
- Cbse Class VI Science: General InstructionsDocumento15 pagineCbse Class VI Science: General InstructionsNaresh world SinghNessuna valutazione finora
- Exercises: Answer 1Documento3 pagineExercises: Answer 1Naresh world SinghNessuna valutazione finora
- The Drugs and Magic Remedies (Objectionable Advertisements) ACT, 1954 - Arrangement of SectionsDocumento8 pagineThe Drugs and Magic Remedies (Objectionable Advertisements) ACT, 1954 - Arrangement of SectionsReetika ShuklaNessuna valutazione finora
- Exercises: Answer 1Documento2 pagineExercises: Answer 1Naresh world SinghNessuna valutazione finora
- Is US Health Really Best in The World PDFDocumento3 pagineIs US Health Really Best in The World PDFpartha9sarathi9ainNessuna valutazione finora
- The Fish Tale: Ans. AnsDocumento7 pagineThe Fish Tale: Ans. AnsNaresh world SinghNessuna valutazione finora
- Exercises: Answer 1Documento2 pagineExercises: Answer 1Naresh world SinghNessuna valutazione finora
- Exercises: Answer 1Documento2 pagineExercises: Answer 1Naresh world Singh100% (1)
- Indian Constitution: The Vision of B. R. Ambedkar: Kamal KumarDocumento8 pagineIndian Constitution: The Vision of B. R. Ambedkar: Kamal KumarNaresh world SinghNessuna valutazione finora
- Tens and Ones: Page No 57Documento5 pagineTens and Ones: Page No 57Naresh world SinghNessuna valutazione finora
- Check SauceDocumento2 pagineCheck Saucebig boss90% (10)
- MasafiDocumento2 pagineMasafiSa LaNessuna valutazione finora
- Funny AcronymsDocumento6 pagineFunny AcronymsSachinvirNessuna valutazione finora
- QP02Documento11 pagineQP02zakwanmustafa0% (1)
- Chapter 1 - Food Quality Control ProgrammeDocumento75 pagineChapter 1 - Food Quality Control ProgrammeFattah Abu Bakar100% (1)
- Legal DraftingDocumento28 pagineLegal Draftingwadzievj100% (1)
- Paper 1 - 2017 EETDocumento10 paginePaper 1 - 2017 EETRayNessuna valutazione finora
- 8th Mode of FinancingDocumento30 pagine8th Mode of FinancingYaseen IqbalNessuna valutazione finora
- Impact of Dust& Dirt Accumulation On The Performance of PV PanelsDocumento4 pagineImpact of Dust& Dirt Accumulation On The Performance of PV PanelserpublicationNessuna valutazione finora
- Government DaoDocumento7 pagineGovernment DaoGevorg A. GalstyanNessuna valutazione finora
- Questionnaire Exercise: Deals Desk Analyst Please Answer Below Questions and Email Your Responses Before First Technical Round of InterviewDocumento2 pagineQuestionnaire Exercise: Deals Desk Analyst Please Answer Below Questions and Email Your Responses Before First Technical Round of InterviewAbhinav SahaniNessuna valutazione finora
- Unpacking and Storage Instruction-EN-0807Documento18 pagineUnpacking and Storage Instruction-EN-0807Tim ZHANGNessuna valutazione finora
- Lampiran Surat 739Documento1 paginaLampiran Surat 739Rap IndoNessuna valutazione finora
- CASA 212 - 200 (NS) : NO Description P.N QTY ConditionDocumento6 pagineCASA 212 - 200 (NS) : NO Description P.N QTY ConditionsssavNessuna valutazione finora
- 2015 Paper 2 Specimen Paper PDFDocumento10 pagine2015 Paper 2 Specimen Paper PDFAhmad Osama MashalyNessuna valutazione finora
- Tran Date Value Date Tran Particular Credit Debit BalanceDocumento96 pagineTran Date Value Date Tran Particular Credit Debit BalanceGenji MaNessuna valutazione finora
- Challenges Students Face in Conducting A Literature ReviewDocumento6 pagineChallenges Students Face in Conducting A Literature ReviewafdtunqhoNessuna valutazione finora
- PlayAGS, Inc.Documento309 paginePlayAGS, Inc.vicr100Nessuna valutazione finora
- BIR Form 2307Documento20 pagineBIR Form 2307Lean Isidro0% (1)
- Nogales V Capitol Medical CenterDocumento2 pagineNogales V Capitol Medical CenterGraceNessuna valutazione finora
- Material DevOps Essentials DEPC enDocumento88 pagineMaterial DevOps Essentials DEPC enCharlineNessuna valutazione finora
- Genetic Engineering AssignmentDocumento20 pagineGenetic Engineering AssignmentAcyl Chloride HaripremNessuna valutazione finora
- Nammcesa 000010 PDFDocumento1.543 pagineNammcesa 000010 PDFBasel Osama RaafatNessuna valutazione finora
- Diagrame Des MomentsDocumento1 paginaDiagrame Des Momentsabdoul ndiayeNessuna valutazione finora
- 2018 Za (Q + Ma) Ac1025Documento95 pagine2018 Za (Q + Ma) Ac1025전민건Nessuna valutazione finora
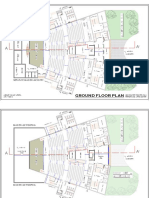
- Abhijit Auditorium Elective Sem 09Documento3 pagineAbhijit Auditorium Elective Sem 09Abhijit Kumar AroraNessuna valutazione finora
- 48 - 1997 SummerDocumento42 pagine48 - 1997 SummerLinda ZwaneNessuna valutazione finora
- The Soyuzist JournalDocumento15 pagineThe Soyuzist Journalcatatonical thingsNessuna valutazione finora
- Marketing Theory and PracticesDocumento4 pagineMarketing Theory and PracticesSarthak RastogiNessuna valutazione finora
- OTDRDocumento57 pagineOTDRarijeetdguy3051100% (1)