Potrebbero piacerti anche
- Improving Access To Care and Community Health in Haiti With Optimized Community Health Worker PlacementDocumento19 pagineImproving Access To Care and Community Health in Haiti With Optimized Community Health Worker Placementh3493061Nessuna valutazione finora
- Admin,+15349 51562 1 CEDocumento7 pagineAdmin,+15349 51562 1 CEh3493061Nessuna valutazione finora
- WFP 0000130513Documento2 pagineWFP 0000130513h3493061Nessuna valutazione finora
- Laboratory Estimation of Rock Joint Stiffness and Frictional ParametersDocumento14 pagineLaboratory Estimation of Rock Joint Stiffness and Frictional Parametersh3493061Nessuna valutazione finora
- Haiti Report PWJ 2Documento5 pagineHaiti Report PWJ 2h3493061Nessuna valutazione finora
- E3sconf Icsree2021 02004Documento7 pagineE3sconf Icsree2021 02004h3493061Nessuna valutazione finora
- Concept Note and Programme2 2Documento5 pagineConcept Note and Programme2 2h3493061Nessuna valutazione finora
- AFI Official Members - Upload On Website - DemoDocumento3 pagineAFI Official Members - Upload On Website - Demoh3493061Nessuna valutazione finora
- Eva Maria Ricardo SlidesDocumento18 pagineEva Maria Ricardo Slidesh3493061Nessuna valutazione finora
- Asia Mozambique Express 20210808 162422Documento9 pagineAsia Mozambique Express 20210808 162422h3493061Nessuna valutazione finora
- Q1: How Will Travelers Be Able To Enter The Country?Documento9 pagineQ1: How Will Travelers Be Able To Enter The Country?h3493061Nessuna valutazione finora
- Mozambique Trade and Investment Factsheet 2021-07-30Documento15 pagineMozambique Trade and Investment Factsheet 2021-07-30h3493061Nessuna valutazione finora
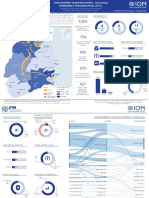
- Emergency Tracking Tool (Ett) : Largest Movements Recorded During The Reporting PeriodDocumento3 pagineEmergency Tracking Tool (Ett) : Largest Movements Recorded During The Reporting Periodh3493061Nessuna valutazione finora
- T - Proc - Notices - Notices - 085 - K - Notice - Doc - 81319 - 170051526Documento9 pagineT - Proc - Notices - Notices - 085 - K - Notice - Doc - 81319 - 170051526h3493061Nessuna valutazione finora
- Wind Star - Tahiti & The Tuamotu Islands 10 Night Cruise On Wind Spirit - Cruise OnlyDocumento7 pagineWind Star - Tahiti & The Tuamotu Islands 10 Night Cruise On Wind Spirit - Cruise Onlyh3493061Nessuna valutazione finora
- PB MW 202107 1Documento3 paginePB MW 202107 1h3493061Nessuna valutazione finora
- Lesotho Japan 50th Anniversary Celebrations UpdatedDocumento4 pagineLesotho Japan 50th Anniversary Celebrations Updatedh3493061Nessuna valutazione finora
- Media Statement. 31 July 2021Documento3 pagineMedia Statement. 31 July 2021h3493061Nessuna valutazione finora
- Scrutinising Multidimensional Challenges in The Maloti-Drakensberg (Lesotho/South Africa)Documento22 pagineScrutinising Multidimensional Challenges in The Maloti-Drakensberg (Lesotho/South Africa)h3493061Nessuna valutazione finora
- Media Statement. 31 July 2021Documento3 pagineMedia Statement. 31 July 2021h3493061Nessuna valutazione finora
- E046633 FullDocumento7 pagineE046633 Fullh3493061Nessuna valutazione finora
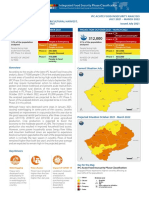
- IPC Lesotho Acute Food Insecurity 2021July2022Mar ReportDocumento7 pagineIPC Lesotho Acute Food Insecurity 2021July2022Mar Reporth3493061Nessuna valutazione finora
- General Information: Fact Sheets Are Updated Biannually August and FebruaryDocumento1 paginaGeneral Information: Fact Sheets Are Updated Biannually August and Februaryh3493061Nessuna valutazione finora
- CY TaxAlerts 6 07 21EN NoexpDocumento2 pagineCY TaxAlerts 6 07 21EN Noexph3493061Nessuna valutazione finora
- Com 2021 398 Cyprus Press Release enDocumento3 pagineCom 2021 398 Cyprus Press Release enh3493061Nessuna valutazione finora
- CYPRUS Reply en Cyprus Newspapers Receive Threats, Cyber-Attacks 02august2021Documento2 pagineCYPRUS Reply en Cyprus Newspapers Receive Threats, Cyber-Attacks 02august2021h3493061Nessuna valutazione finora
- TRIPOLI (LB) Port Schedules-20210707-084210Documento1 paginaTRIPOLI (LB) Port Schedules-20210707-084210h3493061Nessuna valutazione finora
- Cuba: U.S. Policy OverviewDocumento3 pagineCuba: U.S. Policy Overviewh3493061Nessuna valutazione finora
- UK Total Trade Ad-Hoc Data Release Main FDI ReleaseDocumento15 pagineUK Total Trade Ad-Hoc Data Release Main FDI Releaseh3493061Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- CHN - Visit, Bag Technique, EtcDocumento8 pagineCHN - Visit, Bag Technique, EtcAriel Delos ReyesNessuna valutazione finora
- Pamphlet - BurnsDocumento2 paginePamphlet - BurnsOmer ErgeanNessuna valutazione finora
- Cierre de ColostomiaDocumento9 pagineCierre de ColostomiaWildor Herrera GuevaraNessuna valutazione finora
- Sha Fritz 2014Documento10 pagineSha Fritz 2014biancqNessuna valutazione finora
- Research Paper About OintmentDocumento6 pagineResearch Paper About Ointmentpib0b1nisyj2100% (1)
- GP TARIFF With POINT OF CARE TESTS ADDED AND CODESDocumento5 pagineGP TARIFF With POINT OF CARE TESTS ADDED AND CODESAbdulNessuna valutazione finora
- 10th Class English Notes PDF All in OneDocumento15 pagine10th Class English Notes PDF All in Onemuneebnav16Nessuna valutazione finora
- OSHA 300 - Record Keeping DecisionTreeDocumento1 paginaOSHA 300 - Record Keeping DecisionTreeeerrddeemmNessuna valutazione finora
- The Gates of HellDocumento458 pagineThe Gates of Hellmailinglistenator761100% (8)
- TERA-WIRE Dec 19 PDFDocumento27 pagineTERA-WIRE Dec 19 PDFCazz HustlersNessuna valutazione finora
- The Microbiology of Wounds: Neal R. Chamberlain, PH.D., Department of Microbiology/Immunology KcomDocumento31 pagineThe Microbiology of Wounds: Neal R. Chamberlain, PH.D., Department of Microbiology/Immunology KcomFhaliesha Zakur100% (1)
- Osce SuturingDocumento3 pagineOsce Suturingdaniel ragonjanNessuna valutazione finora
- VivaSante - CorporationDocumento15 pagineVivaSante - CorporationFranz OrtegaNessuna valutazione finora
- 2014surgery2 (6 Files Merged)Documento221 pagine2014surgery2 (6 Files Merged)Hannan SyedNessuna valutazione finora
- Medico-Legal Cases: Antipolo City Hospital SystemDocumento39 pagineMedico-Legal Cases: Antipolo City Hospital SystemJDennis CGumpalNessuna valutazione finora
- Pencegahan & Tatalaksana Ulkus DiabetikumDocumento60 paginePencegahan & Tatalaksana Ulkus DiabetikumirhamNessuna valutazione finora
- (SURGERY SGD) Wound HealingDocumento8 pagine(SURGERY SGD) Wound HealingPaulene RiveraNessuna valutazione finora
- Wound Dressings Update: Carolina Weller, Geoff SussmanDocumento7 pagineWound Dressings Update: Carolina Weller, Geoff SussmanKevin AdrianNessuna valutazione finora
- Burn LectureDocumento53 pagineBurn LectureHusna NadiaNessuna valutazione finora
- Care Plan Concept Map - RFIDocumento1 paginaCare Plan Concept Map - RFIsaraNessuna valutazione finora
- Stump Healing in Below Knee Amputations Using Soft Versus Rigid DressingDocumento4 pagineStump Healing in Below Knee Amputations Using Soft Versus Rigid DressingAris Alfaldieka CahyanaNessuna valutazione finora
- People v. Buling YAPDocumento2 paginePeople v. Buling YAPDianne SantiagoNessuna valutazione finora
- Final Concept MapDocumento7 pagineFinal Concept Mapapi-405374041Nessuna valutazione finora
- Nursing Care Plan For HELLP SyndromeDocumento17 pagineNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Fractal Robots Seminar ReportDocumento27 pagineFractal Robots Seminar ReportAkhil ThomasNessuna valutazione finora
- NCPDocumento3 pagineNCPKorina FranciscoNessuna valutazione finora
- 1 First Aid RCS Guide Dec 12Documento28 pagine1 First Aid RCS Guide Dec 12Jade CameronNessuna valutazione finora
- IFU FrontDocumento1 paginaIFU FrontMinh LeNessuna valutazione finora
- Wound Care InstructionsDocumento3 pagineWound Care InstructionsKat TaasinNessuna valutazione finora
- Minor Burns Wound Care: Discharge Information For PatientsDocumento4 pagineMinor Burns Wound Care: Discharge Information For PatientsJoana JohnNessuna valutazione finora