Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- I Had A Hard Time As Finance Minister - Zafrul: Story by DIANA OTHMAN - Yesterday 10:40 PMDocumento2 pagineI Had A Hard Time As Finance Minister - Zafrul: Story by DIANA OTHMAN - Yesterday 10:40 PMHadi Ja'afarNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- MM-M NRP Final Report - April 19th 2022 HadiDocumento488 pagineMM-M NRP Final Report - April 19th 2022 HadiHadi Ja'afarNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Animal Welfare Group MDDB Starts Sponsorship Programme To Raise Funds For The Caring of Its 400 RescuesDocumento3 pagineAnimal Welfare Group MDDB Starts Sponsorship Programme To Raise Funds For The Caring of Its 400 RescuesHadi Ja'afarNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Illegal Settlement Found in A Forest Near Bandar Ainsdale: Story by SYAMILAH ZULKIFLI - Yesterday 9:14 PMDocumento3 pagineIllegal Settlement Found in A Forest Near Bandar Ainsdale: Story by SYAMILAH ZULKIFLI - Yesterday 9:14 PMHadi Ja'afarNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Test of NewsDocumento1 paginaTest of NewsHadi Ja'afarNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
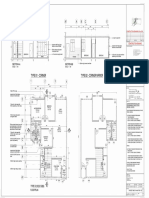
- BBM 1107SQFTDocumento1 paginaBBM 1107SQFTHadi Ja'afarNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Ina ResumeDocumento2 pagineIna ResumeHadi Ja'afarNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Swee Lee Return and Exchange Form Latest Edited VerDocumento2 pagineSwee Lee Return and Exchange Form Latest Edited VerHadi Ja'afarNessuna valutazione finora
- Merchant Name Merchant Order No. FPX Transaction ID Product Description Amount Transaction Status Date & Time Buyer Bank Bank Reference NoDocumento1 paginaMerchant Name Merchant Order No. FPX Transaction ID Product Description Amount Transaction Status Date & Time Buyer Bank Bank Reference NoHadi Ja'afarNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Test PDFDocumento24 pagineTest PDFHadi Ja'afarNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Etiqa Family Takaful Berhad: Dataran Maybank, No. 1, Jalan Maarof, 59000 Kuala Lumpur, MalaysiaDocumento2 pagineEtiqa Family Takaful Berhad: Dataran Maybank, No. 1, Jalan Maarof, 59000 Kuala Lumpur, MalaysiaHadi Ja'afarNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- DuitDocumento1 paginaDuitHadi Ja'afarNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Favourite 3rd Party Transfer: SuccessfulDocumento1 paginaFavourite 3rd Party Transfer: SuccessfulHadi Ja'afarNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Ab 4-7Documento4 pagineAb 4-7api-302561640Nessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Joemari Suba - Mid-Term - Case of KarenDocumento2 pagineJoemari Suba - Mid-Term - Case of KarenJoemari SubaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Oppositional Defiant DisorderDocumento11 pagineOppositional Defiant Disorderbellydanceafrica9540Nessuna valutazione finora
- Obsessive Compulsive DisorderDocumento16 pagineObsessive Compulsive Disorderbelle2602100% (3)
- SCAAREDAdultVersion 1.19.18 PDFDocumento3 pagineSCAAREDAdultVersion 1.19.18 PDFVirvara DanielaNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Mental Health Issues - Documentary VideoDocumento1 paginaMental Health Issues - Documentary VideoJona Mae IberoNessuna valutazione finora
- CBT RebtDocumento2 pagineCBT RebtPriscilla TjjNessuna valutazione finora
- Psychedelic TherapyDocumento3 paginePsychedelic TherapyDarbyWPaulNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Psychology of Perfectionism An Intro PDFDocumento18 pagineThe Psychology of Perfectionism An Intro PDFRobi MaulanaNessuna valutazione finora
- Trauma Focused Art TherapyDocumento18 pagineTrauma Focused Art TherapyMarcosNessuna valutazione finora
- Psychotherapeutic, Somatic and Psychopharmacologic Management Non-Psychotic-PsychoticDocumento7 paginePsychotherapeutic, Somatic and Psychopharmacologic Management Non-Psychotic-PsychoticJo Hn VengzNessuna valutazione finora
- Chapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersDocumento10 pagineChapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersKTNessuna valutazione finora
- Case Report On The JokerDocumento5 pagineCase Report On The Jokersloppyjoes14Nessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Tdah 20Documento14 pagineTdah 20Roberto Alexis Molina CampuzanoNessuna valutazione finora
- MmpiDocumento47 pagineMmpiJohn Alex Saldarriaga25% (4)
- 24th European Congress of Psychiatry / European Psychiatry 33S (2016) S114-S289 S129Documento1 pagina24th European Congress of Psychiatry / European Psychiatry 33S (2016) S114-S289 S129elouchNessuna valutazione finora
- Case Study Mental HealthDocumento11 pagineCase Study Mental Healthapi-402917163Nessuna valutazione finora
- Non-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationDocumento7 pagineNon-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationTututWidyaNurAnggrainiNessuna valutazione finora
- Annual Day 2015 - ProposalDocumento2 pagineAnnual Day 2015 - ProposalAnuradha NagarajanNessuna valutazione finora
- Social PhobiaDocumento11 pagineSocial Phobiakaran_rocks_world709Nessuna valutazione finora
- How To Calm The Agitated Student Intervention CentralDocumento3 pagineHow To Calm The Agitated Student Intervention Centralapi-341096973Nessuna valutazione finora
- Depression Case StudyDocumento2 pagineDepression Case StudyNaga ViewNessuna valutazione finora
- 1000 Plus Psychiatry MCQ Book DranilkakunjeDocumento141 pagine1000 Plus Psychiatry MCQ Book DranilkakunjeChatura UdharaNessuna valutazione finora
- Abnormal BehaviourDocumento25 pagineAbnormal Behaviourfarzana25Nessuna valutazione finora
- Case Study FinalDocumento4 pagineCase Study Finalapi-308562224Nessuna valutazione finora
- Passivity: Aaron Wolfe Schiff, B.A. Jacqui Lee Schiff, M.S.S.WDocumento8 paginePassivity: Aaron Wolfe Schiff, B.A. Jacqui Lee Schiff, M.S.S.WmarijadmNessuna valutazione finora
- What Is Early and First-Episode Psychosis?Documento2 pagineWhat Is Early and First-Episode Psychosis?Frankie VonaNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Deepa SekharDocumento4 pagineDeepa SekharThakur Manu PratapNessuna valutazione finora
- Case Study 1 As Good As It GetsDocumento8 pagineCase Study 1 As Good As It Getsapi-31248710050% (4)
- Level of Anxiety - g5Documento39 pagineLevel of Anxiety - g5Eula Angelica OcoNessuna valutazione finora
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsDa EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsValutazione: 4.5 su 5 stelle4.5/5 (6)