Potrebbero piacerti anche
- Fake Abortion Form TemplateDocumento4 pagineFake Abortion Form Templateyouismyfavcolour67% (3)
- HEC CaseDocumento7 pagineHEC Caseeatonal1801100% (2)
- Tos TemplateDocumento1 paginaTos TemplateIan Bondoc100% (1)
- Tos TemplateDocumento1 paginaTos TemplateIan Bondoc100% (1)
- New Idaho Vaccine Exemption FormDocumento2 pagineNew Idaho Vaccine Exemption FormDonnaNessuna valutazione finora
- UKTB ConsentDocumento2 pagineUKTB ConsentRoha JavidNessuna valutazione finora
- District Aip in DRRM 2019 2020Documento5 pagineDistrict Aip in DRRM 2019 2020Ian Bondoc83% (6)
- Catalog Videos APADocumento28 pagineCatalog Videos APAALEJANDRO MATUTENessuna valutazione finora
- Health Information MatrixDocumento9 pagineHealth Information MatrixVanguardia HighwayNessuna valutazione finora
- Enterprise Architecture StandardsDocumento19 pagineEnterprise Architecture StandardsSmitasamratNessuna valutazione finora
- NY Flu Shot FormDocumento1 paginaNY Flu Shot FormAna AsmaraNessuna valutazione finora
- Flu Vaccine ConsentDocumento2 pagineFlu Vaccine Consentapi-104636361Nessuna valutazione finora
- Flu Consent FormDocumento2 pagineFlu Consent FormTiger Palm TigerNessuna valutazione finora
- Decision To Not Vaccinate My Child: Vaccine / DiseaseDocumento2 pagineDecision To Not Vaccinate My Child: Vaccine / DiseaseNano InnaNessuna valutazione finora
- COVID 19 Consent FormDocumento2 pagineCOVID 19 Consent FormfvdssfdNessuna valutazione finora
- Hospital pg154Documento1 paginaHospital pg154WilliamNessuna valutazione finora
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocumento2 pagineCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNessuna valutazione finora
- COVID-19 Vax Consent FormDocumento3 pagineCOVID-19 Vax Consent FormCj CCNessuna valutazione finora
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Documento4 pagineCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1bersabeh abayNessuna valutazione finora
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocumento1 paginaInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNessuna valutazione finora
- AstraZeneca COVID-19 vaccine informed consentDocumento1 paginaAstraZeneca COVID-19 vaccine informed consentJohn BNessuna valutazione finora
- (ASTRAZENECA) Informed Consent Form - Eng March 5 2021Documento1 pagina(ASTRAZENECA) Informed Consent Form - Eng March 5 2021Mara Ozoa VillaroyaNessuna valutazione finora
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocumento1 paginaInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.Nessuna valutazione finora
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Documento4 pagineRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNessuna valutazione finora
- ImzformDocumento2 pagineImzformapi-509258857Nessuna valutazione finora
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Documento2 pagineFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNessuna valutazione finora
- Medical FormDocumento2 pagineMedical FormHoney AliNessuna valutazione finora
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Documento6 pagineCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Stephanie BewleyNessuna valutazione finora
- Pfizer COVID Vaccine Consent FormDocumento1 paginaPfizer COVID Vaccine Consent FormChristie ConalesNessuna valutazione finora
- YL Camping Consent and Health FormDocumento4 pagineYL Camping Consent and Health Formmcronin1970Nessuna valutazione finora
- Vaccine ExemptionVacLib GeorgiaDocumento2 pagineVaccine ExemptionVacLib GeorgiaDonnaNessuna valutazione finora
- 953b SIPConsentFormSeptember29ENDocumento2 pagine953b SIPConsentFormSeptember29ENMani MNessuna valutazione finora
- Confidential Medical Certificate (Total and Permanent Disability) PDFDocumento3 pagineConfidential Medical Certificate (Total and Permanent Disability) PDFJP PalamNessuna valutazione finora
- BivalentConsent-MichaelBelen-HAG322426Documento2 pagineBivalentConsent-MichaelBelen-HAG322426michaeljohnbelen14Nessuna valutazione finora
- Parental Consent Form-EnGDocumento2 pagineParental Consent Form-EnGMyrna ParasNessuna valutazione finora
- Vaccination Exemption Pursuant To Wisconsin Statute 252.04Documento2 pagineVaccination Exemption Pursuant To Wisconsin Statute 252.04DonnaNessuna valutazione finora
- Consent Form (Sinovac)Documento1 paginaConsent Form (Sinovac)Kresta BenignoNessuna valutazione finora
- COVID-19 Vaccine Screening and ConsentDocumento2 pagineCOVID-19 Vaccine Screening and ConsentGlenn ReinhardtNessuna valutazione finora
- Formulir Klaim Rawat InapDocumento2 pagineFormulir Klaim Rawat InapGoris DonkeyNessuna valutazione finora
- Pfizer Consent Form - FillableDocumento8 paginePfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNessuna valutazione finora
- NMDOH Parental Consent Form for COVID-19 Administration 04162021Documento1 paginaNMDOH Parental Consent Form for COVID-19 Administration 04162021Kristina GarciaNessuna valutazione finora
- BivalentConsent LucianaPedrosopessoa 559154Documento2 pagineBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNessuna valutazione finora
- Ocfs-Medical Statement of Child in ChildcareDocumento2 pagineOcfs-Medical Statement of Child in ChildcareNikki NievesNessuna valutazione finora
- Oregon Immunization CertificateDocumento2 pagineOregon Immunization CertificateJennifer CervelleraNessuna valutazione finora
- ConsentDocumento9 pagineConsentQworldNessuna valutazione finora
- D - Vaccination Minor Consent FormDocumento2 pagineD - Vaccination Minor Consent FormNoemi CamberosNessuna valutazione finora
- Congvax Consent FormDocumento3 pagineCongvax Consent FormRico MaligayaNessuna valutazione finora
- Vaccine Cluster - Health Screening FormDocumento3 pagineVaccine Cluster - Health Screening FormArlene AngelesNessuna valutazione finora
- Secondary FLU Cover Letter E CONSENT HertfordshireDocumento4 pagineSecondary FLU Cover Letter E CONSENT HertfordshireLuz Adriana Ramirez HernandezNessuna valutazione finora
- Intranasal EnglDocumento2 pagineIntranasal Englalondono8595Nessuna valutazione finora
- Your Best Shot at Stopping The FluDocumento2 pagineYour Best Shot at Stopping The FluJayke WilsonNessuna valutazione finora
- Steps Forward Notice of Privacy Practices Acknowledgment FormDocumento2 pagineSteps Forward Notice of Privacy Practices Acknowledgment FormdawnNessuna valutazione finora
- PEDIA Informed Consent Form PfizerDocumento2 paginePEDIA Informed Consent Form PfizerBalba ChrislynNessuna valutazione finora
- Observers Less Than 10 Days Do Not Receive Outlook CredentialsDocumento4 pagineObservers Less Than 10 Days Do Not Receive Outlook CredentialsGeovy YépezNessuna valutazione finora
- Medical Certificate FormDocumento2 pagineMedical Certificate FormFelipeNessuna valutazione finora
- Swine Flu RebuttalDocumento1 paginaSwine Flu Rebuttalinfo3840Nessuna valutazione finora
- Permission For Child To Participate in ActivityDocumento1 paginaPermission For Child To Participate in ActivityLegal FormsNessuna valutazione finora
- Anthrax Vaccine:: What You Need To KnowDocumento2 pagineAnthrax Vaccine:: What You Need To KnowThadNessuna valutazione finora
- Hospitalization Reimbursment Claim FormDocumento4 pagineHospitalization Reimbursment Claim FormFarhan aliNessuna valutazione finora
- FAQ COVID Vaccines for Families & EducatorsDocumento2 pagineFAQ COVID Vaccines for Families & EducatorsLizzie Hernández-CarrizalesNessuna valutazione finora
- COVID-19 Consent FormDocumento1 paginaCOVID-19 Consent FormAshley PowerNessuna valutazione finora
- Flu Clinic Admin Record 2022Documento2 pagineFlu Clinic Admin Record 2022MATTHEW JONESNessuna valutazione finora
- C&a Consent FormsDocumento28 pagineC&a Consent Formsjgcj477rh9Nessuna valutazione finora
- DO PBL Paper Case 16 HIV OSCEDocumento4 pagineDO PBL Paper Case 16 HIV OSCESmelly RaccoonNessuna valutazione finora
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocumento2 pagineConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNessuna valutazione finora
- Certificate of Accuracy For "HIV" Antibody TestingDocumento2 pagineCertificate of Accuracy For "HIV" Antibody Testingtomasbrewster2409Nessuna valutazione finora
- Influenza Vaccine (Influvac) Consent Form: Title: Name: Age: GenderDocumento1 paginaInfluenza Vaccine (Influvac) Consent Form: Title: Name: Age: GenderIan BondocNessuna valutazione finora
- Department of Education: Individual Workweek Accomplishment ReportDocumento8 pagineDepartment of Education: Individual Workweek Accomplishment ReportIan BondocNessuna valutazione finora
- Department of Education: Dolores Piring Elementary SchoolDocumento5 pagineDepartment of Education: Dolores Piring Elementary SchoolIan BondocNessuna valutazione finora
- Sample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Documento5 pagineSample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Ian BondocNessuna valutazione finora
- Sample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Documento5 pagineSample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Ian BondocNessuna valutazione finora
- Division of Pampanga: Brigada Eskwela 2020 District/Cluster Consolidated ReportDocumento1 paginaDivision of Pampanga: Brigada Eskwela 2020 District/Cluster Consolidated ReportIan BondocNessuna valutazione finora
- Individual Workweek Accomplishment PlanDocumento1 paginaIndividual Workweek Accomplishment Planbernadeth villanuevaNessuna valutazione finora
- Individual Workweek Accomplishment PlanDocumento1 paginaIndividual Workweek Accomplishment Planbernadeth villanuevaNessuna valutazione finora
- DepEd Email Account Details and Activation InstructionsDocumento1 paginaDepEd Email Account Details and Activation InstructionsIan BondocNessuna valutazione finora
- Incoming Grade 6 Part C and D of Lesf SurveyDocumento1.356 pagineIncoming Grade 6 Part C and D of Lesf SurveyIan BondocNessuna valutazione finora
- Curriculum Implementation Division (CID) : This Material Was Contextualized by TheDocumento1 paginaCurriculum Implementation Division (CID) : This Material Was Contextualized by TheIan BondocNessuna valutazione finora
- Lesson Exemplar Science 4 Template 2019Documento6 pagineLesson Exemplar Science 4 Template 2019Dolores EspinosaNessuna valutazione finora
- Acknowledgment Receipt for Borrower Protection PlanDocumento2 pagineAcknowledgment Receipt for Borrower Protection PlanCyrell Castroverde PapauranNessuna valutazione finora
- Division of Pampanga: Brigada Eskwela 2020 District/Cluster Consolidated ReportDocumento1 paginaDivision of Pampanga: Brigada Eskwela 2020 District/Cluster Consolidated ReportIan BondocNessuna valutazione finora
- Kagawaran NG Edukasyon: Juan Dela CruzDocumento2 pagineKagawaran NG Edukasyon: Juan Dela CruzIan BondocNessuna valutazione finora
- Sample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Documento5 pagineSample Teacher Individual Workweek Plan Accomplishment Sy 2020 2021 1Ian BondocNessuna valutazione finora
- Classroom Action ResearchDocumento10 pagineClassroom Action ResearchIan BondocNessuna valutazione finora
- Lesson Exemplar Science 4 Template 2019Documento6 pagineLesson Exemplar Science 4 Template 2019Dolores EspinosaNessuna valutazione finora
- Dpes SPG June Drug SymposiumDocumento5 pagineDpes SPG June Drug SymposiumIan BondocNessuna valutazione finora
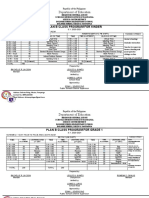
- Department of Educa: Plan B Class Program For KinderDocumento8 pagineDepartment of Educa: Plan B Class Program For KinderIan BondocNessuna valutazione finora
- Supreme Pupil Government 2018-2019 List of Officers: Dolores Piring Elementary SchoolDocumento11 pagineSupreme Pupil Government 2018-2019 List of Officers: Dolores Piring Elementary SchoolIan BondocNessuna valutazione finora
- Strategic Intervention Materials Evaluation CriteriaDocumento1 paginaStrategic Intervention Materials Evaluation CriteriaIan BondocNessuna valutazione finora
- Brigada Eskwela Action Plan: Tañong National High SchoolDocumento4 pagineBrigada Eskwela Action Plan: Tañong National High SchoolmelyNessuna valutazione finora
- SIMs Strategic Intervention Materials CRITERIADocumento1 paginaSIMs Strategic Intervention Materials CRITERIAIan BondocNessuna valutazione finora
- Grade School Science Syllabus Explains Branches, ImportanceDocumento33 pagineGrade School Science Syllabus Explains Branches, ImportanceIan BondocNessuna valutazione finora
- Mexico Elementary School: School Consolidated Group Screening Test (English)Documento2 pagineMexico Elementary School: School Consolidated Group Screening Test (English)Ian BondocNessuna valutazione finora
- Surgical Audit and Peer Review Guide 2014Documento54 pagineSurgical Audit and Peer Review Guide 2014juweriyNessuna valutazione finora
- Disaster Continuum: Scaling The Heights of Flexible LearningDocumento25 pagineDisaster Continuum: Scaling The Heights of Flexible LearningKRIZIA ANE A. SULONGNessuna valutazione finora
- CertificateDocumento1 paginaCertificaterinku kushwahNessuna valutazione finora
- QSE Candidate Information HandbookDocumento17 pagineQSE Candidate Information HandbookAlex RosianNessuna valutazione finora
- Principles of Research Ethics: Prepared By: Assist. Prof. Dr. Yassin A. AsaadDocumento19 paginePrinciples of Research Ethics: Prepared By: Assist. Prof. Dr. Yassin A. AsaadasdfsNessuna valutazione finora
- RN Claims Risk Manager in Phoenix AZ Resume Candace CouchDocumento2 pagineRN Claims Risk Manager in Phoenix AZ Resume Candace CouchCandace CouchNessuna valutazione finora
- NPPCD GuidelinesDocumento10 pagineNPPCD GuidelinesRs WsNessuna valutazione finora
- Pengertian Kredensialing dan Kewenangan Klinis untuk Staf MedisDocumento39 paginePengertian Kredensialing dan Kewenangan Klinis untuk Staf MedisIndri TriantikaNessuna valutazione finora
- Fy 2018 Malawi Malaria Operational PlanDocumento81 pagineFy 2018 Malawi Malaria Operational PlanMochamad Aldy HusenNessuna valutazione finora
- Administering Intradermal Injection Skin TestDocumento2 pagineAdministering Intradermal Injection Skin TestKrysstal GerongaNessuna valutazione finora
- 2016) - The Definition, Diagnostic Testing, and Management of Chronic Inducible Urticarias-The EAACIGA 2 LENEDFUNEV Consensus Recommendations 2016 Update and Revision.Documento23 pagine2016) - The Definition, Diagnostic Testing, and Management of Chronic Inducible Urticarias-The EAACIGA 2 LENEDFUNEV Consensus Recommendations 2016 Update and Revision.elçinNessuna valutazione finora
- PHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Documento228 paginePHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Tanvir Ahmed NayeemNessuna valutazione finora
- Effect of Prone Positioning on Respiratory Rate and Oxygen Saturation in Infants with RDSDocumento3 pagineEffect of Prone Positioning on Respiratory Rate and Oxygen Saturation in Infants with RDSAgustina VivoNessuna valutazione finora
- Sector Grant and Budget Guidelines 2017/18Documento152 pagineSector Grant and Budget Guidelines 2017/18NsubugaNessuna valutazione finora
- Benefits of CounsellingDocumento2 pagineBenefits of CounsellingJc OnyekwereNessuna valutazione finora
- Healthcare White PaperDocumento13 pagineHealthcare White PaperJacobPersily100% (1)
- 5574 16255 1 PBDocumento5 pagine5574 16255 1 PBDwi SeftiNessuna valutazione finora
- Reimagining The Possible in The Indian Healthcare Ecosystem With Emerging TechnologiesDocumento21 pagineReimagining The Possible in The Indian Healthcare Ecosystem With Emerging TechnologiesswarnaNessuna valutazione finora
- Botanical PharmacognosyDocumento6 pagineBotanical PharmacognosycoloromaneNessuna valutazione finora
- Buku English For MidwiferyDocumento31 pagineBuku English For MidwiferyMiss Hanay VinnyNessuna valutazione finora
- Say Goodbye To Your Bad Health Through CuppingDocumento23 pagineSay Goodbye To Your Bad Health Through CuppingTameem AhmedNessuna valutazione finora
- Your Essential Guide To Canada: What You Need To Know To Make Your Relocation Smooth and SuccessfulDocumento55 pagineYour Essential Guide To Canada: What You Need To Know To Make Your Relocation Smooth and SuccessfulxxavierNessuna valutazione finora
- COVID Vaccination Certificate for Jitendra MahajanDocumento1 paginaCOVID Vaccination Certificate for Jitendra MahajansumandeepNessuna valutazione finora
- Using Marsh Scores To Diagnose Celiac DiseaseDocumento1 paginaUsing Marsh Scores To Diagnose Celiac DiseaseSandra PetkovskaNessuna valutazione finora
- RNTCP Treatment GuidelinesDocumento43 pagineRNTCP Treatment GuidelinesSanket AgrawalNessuna valutazione finora
- MPT SyllabusDocumento27 pagineMPT SyllabusvinaymanNessuna valutazione finora