Potrebbero piacerti anche
- Introduction To Pharmaceutical MicrobiologyDocumento35 pagineIntroduction To Pharmaceutical MicrobiologylorrainebarandonNessuna valutazione finora
- Blood Transfusion Services Strengthen Maternal HealthDocumento19 pagineBlood Transfusion Services Strengthen Maternal HealthJOSHUA DICHOSONessuna valutazione finora
- GE 8 Ethics PESTLE AnalysisDocumento3 pagineGE 8 Ethics PESTLE AnalysisJOSHUA DICHOSONessuna valutazione finora
- CHN ConceptsDocumento48 pagineCHN ConceptsJOSHUA DICHOSONessuna valutazione finora
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDocumento2 pagineCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONessuna valutazione finora
- Philippines Commitment Self-Reporting Questionnaire 2018Documento7 paginePhilippines Commitment Self-Reporting Questionnaire 2018JOSHUA DICHOSONessuna valutazione finora
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDocumento19 pagineAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONessuna valutazione finora
- (.-..-.)Documento1 pagina(.-..-.)JOSHUA DICHOSONessuna valutazione finora
- Kawasaki Disease-Case-Study LATEST CHANGESDocumento24 pagineKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- Case PresentationDocumento39 pagineCase PresentationJOSHUA DICHOSONessuna valutazione finora
- Which of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsDocumento2 pagineWhich of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsJOSHUA DICHOSONessuna valutazione finora
- Pneumonia Presenting as Acute Abdomen in ChildrenDocumento4 paginePneumonia Presenting as Acute Abdomen in ChildrenJOSHUA DICHOSONessuna valutazione finora
- Physiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFDocumento15 paginePhysiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFnurulanisa0703Nessuna valutazione finora
- Recommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseDocumento34 pagineRecommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseJOSHUA DICHOSONessuna valutazione finora
- 6234-Article Text-8420-2-10-20170221Documento3 pagine6234-Article Text-8420-2-10-20170221Jenry Himawan SinagaNessuna valutazione finora
- 3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsDocumento12 pagine3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsJOSHUA DICHOSONessuna valutazione finora
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDocumento2 pagineCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONessuna valutazione finora
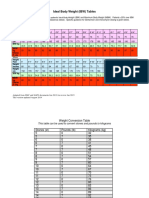
- IBW TableDocumento2 pagineIBW TablegrafikeyesNessuna valutazione finora
- Nursing Interventions and Rationales - Impaired Skin IntegrityDocumento11 pagineNursing Interventions and Rationales - Impaired Skin IntegrityJOSHUA DICHOSONessuna valutazione finora
- P롶허ㅓㅠㄹ포ㅗ)Documento19 pagineP롶허ㅓㅠㄹ포ㅗ)JOSHUA DICHOSONessuna valutazione finora
- How To Study Pharmacology Checklist Cheat SheetDocumento4 pagineHow To Study Pharmacology Checklist Cheat SheetJOSHUA DICHOSONessuna valutazione finora
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDocumento19 pagineAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONessuna valutazione finora
- Tobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsDocumento104 pagineTobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsJOSHUA DICHOSONessuna valutazione finora
- Patient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)Documento28 paginePatient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)JOSHUA DICHOSO100% (1)
- Introduction PDFDocumento1 paginaIntroduction PDFJOSHUA DICHOSONessuna valutazione finora
- Agency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3Documento2 pagineAgency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3JOSHUA DICHOSONessuna valutazione finora
- Preventing Skin Damage and Pressure UlcersDocumento29 paginePreventing Skin Damage and Pressure UlcersJOSHUA DICHOSO100% (1)
- De Nition: Chapter 46 Chest ExaminationDocumento7 pagineDe Nition: Chapter 46 Chest ExaminationJOSHUA DICHOSONessuna valutazione finora
- Nursing Care Plans Made EasyDocumento23 pagineNursing Care Plans Made EasyJOSHUA DICHOSONessuna valutazione finora
- Course Syllabus: Course: Hours: Course DescriptionDocumento10 pagineCourse Syllabus: Course: Hours: Course DescriptionJOSHUA DICHOSONessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- New Directions in The Treatment of HypoparathyroidismDocumento6 pagineNew Directions in The Treatment of Hypoparathyroidismmiguel saba sabaNessuna valutazione finora
- Age Related White Matter and Gray Matter ChangesDocumento11 pagineAge Related White Matter and Gray Matter ChangesJuan José Figueroa ValdiviezoNessuna valutazione finora
- HEALTHY JUICES AND THEIR BENEFITSDocumento9 pagineHEALTHY JUICES AND THEIR BENEFITSGertrude QuaicoeNessuna valutazione finora
- Radio Show Planning BookletDocumento5 pagineRadio Show Planning Bookletapi-576726761Nessuna valutazione finora
- Sildenafil Citrate or ViagraDocumento3 pagineSildenafil Citrate or ViagraKat ZNessuna valutazione finora
- IMCI Orientation Powerpoint PresentationDocumento45 pagineIMCI Orientation Powerpoint Presentationboynegro100% (18)
- Magnetic Resonance ImagingDocumento8 pagineMagnetic Resonance ImagingPrajwal S Kotyan PskNessuna valutazione finora
- AARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013Documento10 pagineAARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013jvalenciagNessuna valutazione finora
- DPWH Department Order No. 030 Series of 2021Documento12 pagineDPWH Department Order No. 030 Series of 2021Carissa Mae RemondeNessuna valutazione finora
- Myasthenia Gravis: MG-epidemiologyDocumento3 pagineMyasthenia Gravis: MG-epidemiologyRemigius RiyanNessuna valutazione finora
- High-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable OnlineDocumento12 pagineHigh-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable Onlinejeinzen14Nessuna valutazione finora
- 2015 To 2019 Super Speciality Dissertation Topics PDFDocumento35 pagine2015 To 2019 Super Speciality Dissertation Topics PDFJoseph John Crasto100% (2)
- ARAV Trifold Ball Pythonv2 2Documento2 pagineARAV Trifold Ball Pythonv2 2rastogishlok04Nessuna valutazione finora
- Refusing To Imagine? On The Possibility of Psychogenic AphantasiaDocumento3 pagineRefusing To Imagine? On The Possibility of Psychogenic AphantasiaSAMUEL SALAZAR MURILLONessuna valutazione finora
- Chap-2 Notes For Clinical Nutrition and DieteticsDocumento5 pagineChap-2 Notes For Clinical Nutrition and Dieteticsstar “Hjaljimmer” platinumNessuna valutazione finora
- Primary Health CareDocumento17 paginePrimary Health CareKevins ChepsirNessuna valutazione finora
- Hemo Flagellate SDocumento13 pagineHemo Flagellate Sgwyne agdipaNessuna valutazione finora
- Sleep Study ThesisDocumento5 pagineSleep Study Thesisamandasanchezalbuquerque100% (2)
- Harish Vinayak Kuber: Glenmark Pharmaceuticals LTDDocumento281 pagineHarish Vinayak Kuber: Glenmark Pharmaceuticals LTDTIMEPASS CAPTURENessuna valutazione finora
- Prescription of Exercise in Older Adults Physiotherapeutic ApproachDocumento4 paginePrescription of Exercise in Older Adults Physiotherapeutic ApproachMaría José Suero RodríguezNessuna valutazione finora
- Cardiology 7 - Arrhythmias: Lecture OutlineDocumento6 pagineCardiology 7 - Arrhythmias: Lecture Outlineمحمد احمد محمدNessuna valutazione finora
- Decoding The Whispers of DerpressionDocumento17 pagineDecoding The Whispers of DerpressionMickoy D. EbagagNessuna valutazione finora
- Establish and Maintain Whs Safety System1Documento46 pagineEstablish and Maintain Whs Safety System1raj ramukNessuna valutazione finora
- Annals of The New York Academy of Sciences - 2023 - Hess - Accelerating Action To Reduce Anemia Review of Causes and RiskDocumento13 pagineAnnals of The New York Academy of Sciences - 2023 - Hess - Accelerating Action To Reduce Anemia Review of Causes and RiskIdmNessuna valutazione finora
- 22 Pool Safety Operating Procedure Jan 2015Documento8 pagine22 Pool Safety Operating Procedure Jan 2015Surf Life Saving MauritiusNessuna valutazione finora
- 10.1016/j.ymgme.2016.11.045: Abstracts / Molecular Genetics and Metabolism 120 (2016) S17 - S145 S29Documento2 pagine10.1016/j.ymgme.2016.11.045: Abstracts / Molecular Genetics and Metabolism 120 (2016) S17 - S145 S29Larisa IliescuNessuna valutazione finora
- Pharma Nursing ApplicationDocumento53 paginePharma Nursing ApplicationRiegne Chiara Fay AcuzarNessuna valutazione finora
- Zika y EmbarazoDocumento10 pagineZika y EmbarazoSMIBA MedicinaNessuna valutazione finora
- 3 Chemical Examination of UrineDocumento82 pagine3 Chemical Examination of UrineJake Real Dela RocaNessuna valutazione finora
- DiseasesofAnimals DiagnosisandManagementDocumento177 pagineDiseasesofAnimals DiagnosisandManagementDr Ankit yadavNessuna valutazione finora