Potrebbero piacerti anche
- Anchored: How to Befriend Your Nervous System Using Polyvagal TheoryDa EverandAnchored: How to Befriend Your Nervous System Using Polyvagal TheoryValutazione: 5 su 5 stelle5/5 (3)
- NCP Anxiety PretermDocumento1 paginaNCP Anxiety Pretermanreilegarde89% (9)
- Armed Services Medication ListDocumento227 pagineArmed Services Medication Listpaulsaint68100% (1)
- 2 - EndometriosisDocumento3 pagine2 - EndometriosisJayson Olile100% (1)
- Crash Course - General PharmacologyDocumento62 pagineCrash Course - General PharmacologyDhanesh VijayaraghavanNessuna valutazione finora
- Handbook of Palliative Medicine in MalaysiaDocumento95 pagineHandbook of Palliative Medicine in Malaysiaumiraihana1Nessuna valutazione finora
- Analgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Documento10 pagineAnalgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Juan ParedesNessuna valutazione finora
- Ananad2 PDFDocumento8 pagineAnanad2 PDFmustafasacarNessuna valutazione finora
- Paediatrics Pain ManagementDocumento9 paginePaediatrics Pain Managementfuka priesleyNessuna valutazione finora
- .Dolor Neonato TradDocumento10 pagine.Dolor Neonato TradAsdrubal MontañoNessuna valutazione finora
- A Review of Pain Management in The Neonate: Evidence-Based Pharmacy PracticeDocumento4 pagineA Review of Pain Management in The Neonate: Evidence-Based Pharmacy PracticeAndriy SubieNessuna valutazione finora
- N.P. of LscsDocumento8 pagineN.P. of LscsHarish LabanaNessuna valutazione finora
- Fetal FiskDocumento5 pagineFetal FiskHernán AlvarezNessuna valutazione finora
- Chronic Stress Cortisol Dysfunction and PainDocumento10 pagineChronic Stress Cortisol Dysfunction and PainMomna KashifNessuna valutazione finora
- Role of Psychology in Pain Management 2001Documento9 pagineRole of Psychology in Pain Management 2001MilenaSpasovskaNessuna valutazione finora
- 2014 Chronic Pain. The Role of Learning and Brain PlasticityDocumento12 pagine2014 Chronic Pain. The Role of Learning and Brain PlasticityCristian OyarzoNessuna valutazione finora
- Eview Article: Pain Relief in NeonatesDocumento9 pagineEview Article: Pain Relief in NeonatesresidenanakNessuna valutazione finora
- The Discomfort of Labor: Pailz and and BirthDocumento11 pagineThe Discomfort of Labor: Pailz and and BirthIhwan ZoffonNessuna valutazione finora
- Intrapartum Pain Management ReviewerDocumento5 pagineIntrapartum Pain Management ReviewerCamille Coruña AranteNessuna valutazione finora
- LutzAlteredNeuroImage PDFDocumento9 pagineLutzAlteredNeuroImage PDFPao ManriqueNessuna valutazione finora
- Grant NYAS 2014Documento9 pagineGrant NYAS 2014grantj8Nessuna valutazione finora
- Pain ManagementDocumento5 paginePain ManagementHany ElbarougyNessuna valutazione finora
- Perinatal Depression: A ReviewDocumento5 paginePerinatal Depression: A ReviewDewi NofiantiNessuna valutazione finora
- Perinatal Depression Review 20Documento5 paginePerinatal Depression Review 20Paula SouzaNessuna valutazione finora
- NCP Acute Pain Related To InflammationDocumento3 pagineNCP Acute Pain Related To InflammationMa. Elaine Carla Tating38% (8)
- Fundamentals of Nursing Practice #16Documento8 pagineFundamentals of Nursing Practice #16AS DeltaNessuna valutazione finora
- Prevention and Management of Procedural Pain in The Neonate An U 2016Documento13 paginePrevention and Management of Procedural Pain in The Neonate An U 2016Indra WijayaNessuna valutazione finora
- Review Oxford Textbook of Pediatric Pain: August 2021Documento3 pagineReview Oxford Textbook of Pediatric Pain: August 2021rehabaya 2022Nessuna valutazione finora
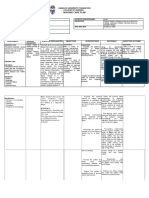
- Assessment Diagnosis Background Knowledge Planning Intervention Rationale Evaluation SubjectiveDocumento3 pagineAssessment Diagnosis Background Knowledge Planning Intervention Rationale Evaluation SubjectiveAngelaNessuna valutazione finora
- Dienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDocumento11 pagineDienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDienizs Labini TadenaNessuna valutazione finora
- Altered Sensorium Batch 2016Documento9 pagineAltered Sensorium Batch 2016Adriel PagariganNessuna valutazione finora
- Nursing Care Plan Age: 60 Years OldDocumento4 pagineNursing Care Plan Age: 60 Years OldLouise GudmalinNessuna valutazione finora
- Evid Based Nurs 2012 Meek 84 5Documento3 pagineEvid Based Nurs 2012 Meek 84 5Sasha Hidayat FullNessuna valutazione finora
- Dienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDocumento11 pagineDienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDienizs Labini TadenaNessuna valutazione finora
- Nursing Care Plan On FatigueDocumento5 pagineNursing Care Plan On FatigueMelvin D. RamosNessuna valutazione finora
- Pain Management in ChildrenDocumento19 paginePain Management in ChildrenNeo SamontinaNessuna valutazione finora
- 4 U1.0 B978 0 7216 9654 6..50177 6..DOCPDFDocumento5 pagine4 U1.0 B978 0 7216 9654 6..50177 6..DOCPDFgilmeraf2000Nessuna valutazione finora
- CPH 2ND WK NCPDocumento5 pagineCPH 2ND WK NCPAyessa Camelle DumileNessuna valutazione finora
- Postoperative Analgesia in Infants and Children: P.-A. Lo Nnqvist and N. S. MortonDocumento10 paginePostoperative Analgesia in Infants and Children: P.-A. Lo Nnqvist and N. S. MortonMega SudibiaNessuna valutazione finora
- Paloayen Mod12 NCPDocumento4 paginePaloayen Mod12 NCPAyen PaloNessuna valutazione finora
- 793 Full PDFDocumento7 pagine793 Full PDFPoliana carmonaNessuna valutazione finora
- Anesthesia and Analgesia in The NICUDocumento19 pagineAnesthesia and Analgesia in The NICUPaulHerreraNessuna valutazione finora
- The Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesDocumento10 pagineThe Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesmustafasacarNessuna valutazione finora
- A Systematic Review of Sleep in Pediatric Pain PopulationsDocumento16 pagineA Systematic Review of Sleep in Pediatric Pain Populationsveigaarthur84Nessuna valutazione finora
- Paediatric Sedation: Michael R. J. Sury FRCADocumento5 paginePaediatric Sedation: Michael R. J. Sury FRCASantosa TandiNessuna valutazione finora
- Finals Notes UnfinishedDocumento23 pagineFinals Notes UnfinishedNicholeGarcesCisnerosNessuna valutazione finora
- 2017 A Neurobiologist's Attempt To Understand Persistent PainDocumento8 pagine2017 A Neurobiologist's Attempt To Understand Persistent PainCristian OyarzoNessuna valutazione finora
- Psychological Interventions For Acute Pediatric Pain: Christina Liossi and Linda S FranckDocumento16 paginePsychological Interventions For Acute Pediatric Pain: Christina Liossi and Linda S FranckbangkitayuNessuna valutazione finora
- Practical Approach To Analgesia and SedaDocumento8 paginePractical Approach To Analgesia and SedaRAGHU NATH KARMAKERNessuna valutazione finora
- Postoperative Analgesia in Infants and Children: P.-A. Lo Nnqvist and N. S. MortonDocumento10 paginePostoperative Analgesia in Infants and Children: P.-A. Lo Nnqvist and N. S. MortonT RonaskyNessuna valutazione finora
- Appendicitis NCPDocumento5 pagineAppendicitis NCPEarl Joseph DezaNessuna valutazione finora
- Appendicitis - NCPDocumento5 pagineAppendicitis - NCPEarl Joseph Deza100% (1)
- Idc NCPDocumento14 pagineIdc NCPEnrique BabierraNessuna valutazione finora
- Pain Basic Consideration PDFDocumento4 paginePain Basic Consideration PDFCiprian CorneaNessuna valutazione finora
- 06 Jaworska-Andryszewska2019Documento9 pagine06 Jaworska-Andryszewska2019DigsNessuna valutazione finora
- Group 1 1Documento6 pagineGroup 1 1SeeTheKing WalkerNessuna valutazione finora
- Dolor en NiñosDocumento14 pagineDolor en NiñospatNessuna valutazione finora
- Conscious Sedation PaediatricsDocumento44 pagineConscious Sedation PaediatricsReeta TaxakNessuna valutazione finora
- NCPDocumento4 pagineNCPJhuRise Ann ManganaNessuna valutazione finora
- 1 NCPDocumento3 pagine1 NCPNicole Mendonis LunarNessuna valutazione finora
- Nursing Care Plan On FatigueDocumento5 pagineNursing Care Plan On FatigueMelvin D. RamosNessuna valutazione finora
- Parenting: The Art and Science of Teaching Your Baby to Sleep (Overcome Past Trauma Face Abandonment and Regain Emotional Stability)Da EverandParenting: The Art and Science of Teaching Your Baby to Sleep (Overcome Past Trauma Face Abandonment and Regain Emotional Stability)Nessuna valutazione finora
- Reversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)Da EverandReversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)Nessuna valutazione finora
- Accuracy and Outcome of Mandibular Fracture Reduction Without and With An Aid of A Repositioning ForcepsDocumento8 pagineAccuracy and Outcome of Mandibular Fracture Reduction Without and With An Aid of A Repositioning ForcepsmustafasacarNessuna valutazione finora
- Mandible Fractures: Brent B. Pickrell, MD Arman T. Serebrakian, MD, MS Renata S. Maricevich, MDDocumento8 pagineMandible Fractures: Brent B. Pickrell, MD Arman T. Serebrakian, MD, MS Renata S. Maricevich, MDmustafasacarNessuna valutazione finora
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocumento31 pagineWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsmustafasacarNessuna valutazione finora
- Fixation of Mandibular Angle Fractures: in Vitro Biomechanical Assessments and Computer-Based StudiesDocumento19 pagineFixation of Mandibular Angle Fractures: in Vitro Biomechanical Assessments and Computer-Based StudiesmustafasacarNessuna valutazione finora
- Changing Trends in The Treatment of Mandibular Fracture: Mohammad Waheed El-AnwarDocumento2 pagineChanging Trends in The Treatment of Mandibular Fracture: Mohammad Waheed El-AnwarmustafasacarNessuna valutazione finora
- 10 Jpts 27 1455Documento3 pagine10 Jpts 27 1455mustafasacarNessuna valutazione finora
- 6-Effects of Kinesiology Taping in Children With CerDocumento10 pagine6-Effects of Kinesiology Taping in Children With CermustafasacarNessuna valutazione finora
- CeelieDocumento6 pagineCeeliemustafasacarNessuna valutazione finora
- Epidemiology and Treatment of Painful Procedures in Neonates in Intensive Care UnitsDocumento13 pagineEpidemiology and Treatment of Painful Procedures in Neonates in Intensive Care UnitsmustafasacarNessuna valutazione finora
- The Effectiveness of Taping On Children With Cerebral Palsy: A Systematic ReviewDocumento5 pagineThe Effectiveness of Taping On Children With Cerebral Palsy: A Systematic ReviewmustafasacarNessuna valutazione finora
- Prolonged Sedation And/or Analgesia and 5-Year Neurodevelopment Outcome in Very Preterm InfantsDocumento6 pagineProlonged Sedation And/or Analgesia and 5-Year Neurodevelopment Outcome in Very Preterm InfantsmustafasacarNessuna valutazione finora
- 3 13059 ArticleText 24188 2 10 20191119Documento9 pagine3 13059 ArticleText 24188 2 10 20191119mustafasacarNessuna valutazione finora
- Blood Sampling in Infants (Reducing Pain and Morbidity) : Olga KapellouDocumento18 pagineBlood Sampling in Infants (Reducing Pain and Morbidity) : Olga KapelloumustafasacarNessuna valutazione finora
- Summary Proceedings From The Neonatal Pain-Control Group: Supplement ArticleDocumento16 pagineSummary Proceedings From The Neonatal Pain-Control Group: Supplement ArticlemustafasacarNessuna valutazione finora
- Carbajal 2 PDFDocumento5 pagineCarbajal 2 PDFmustafasacarNessuna valutazione finora
- Stevens2 PDFDocumento362 pagineStevens2 PDFmustafasacarNessuna valutazione finora
- A Systematic Review of Lidocaine-Prilocaine Cream (EMLA) in The Treatment of Acute Pain in NeonatesDocumento11 pagineA Systematic Review of Lidocaine-Prilocaine Cream (EMLA) in The Treatment of Acute Pain in NeonatesmustafasacarNessuna valutazione finora
- In The: Evidence ForDocumento7 pagineIn The: Evidence FormustafasacarNessuna valutazione finora
- The Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesDocumento10 pagineThe Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesmustafasacarNessuna valutazione finora
- sTEVENS PDFDocumento9 paginesTEVENS PDFmustafasacarNessuna valutazione finora
- Sexton PDFDocumento5 pagineSexton PDFmustafasacarNessuna valutazione finora
- Development and Initial Validation of The EDIN Scale, A New Tool For Assessing Prolonged Pain in Preterm InfantsDocumento6 pagineDevelopment and Initial Validation of The EDIN Scale, A New Tool For Assessing Prolonged Pain in Preterm InfantsmustafasacarNessuna valutazione finora
- Clinical Study: COVERS Neonatal Pain Scale: Development and ValidationDocumento5 pagineClinical Study: COVERS Neonatal Pain Scale: Development and ValidationmustafasacarNessuna valutazione finora
- Theories of Pain: From Specificity To Gate Control: ReviewDocumento8 pagineTheories of Pain: From Specificity To Gate Control: ReviewmustafasacarNessuna valutazione finora
- Sucrose For Procedural Pain Management in Infants: AuthorsDocumento10 pagineSucrose For Procedural Pain Management in Infants: AuthorsmustafasacarNessuna valutazione finora
- Kaynak RADocumento1 paginaKaynak RAmustafasacarNessuna valutazione finora
- DurrmeyerDocumento11 pagineDurrmeyermustafasacarNessuna valutazione finora
- Analgesic Property of Corchorus Olitorius LDocumento52 pagineAnalgesic Property of Corchorus Olitorius LabdallahlotfylNessuna valutazione finora
- Common Drugs and Antidotes: Substance AntidoteDocumento2 pagineCommon Drugs and Antidotes: Substance AntidoteJo Ellie MarfilNessuna valutazione finora
- S 006 LBLDocumento21 pagineS 006 LBLEko YuliantoNessuna valutazione finora
- CNU-CN FORM 002 Cebu Normal University College of Nursing CebuDocumento15 pagineCNU-CN FORM 002 Cebu Normal University College of Nursing Ceburyuka123Nessuna valutazione finora
- Epidemiology and Definition: o Most Common Locations: o Acute PainDocumento4 pagineEpidemiology and Definition: o Most Common Locations: o Acute PainJudy Ignacio EclarinoNessuna valutazione finora
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocumento5 pagineMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNessuna valutazione finora
- Acetaminophen Properties Clinical Uses and Adverse Effects PDFDocumento218 pagineAcetaminophen Properties Clinical Uses and Adverse Effects PDFmirza_baig_46Nessuna valutazione finora
- Kawasaki DiseaseDocumento14 pagineKawasaki Diseaseken100% (2)
- Policy On Pediatric Dental Pain ManagementDocumento3 paginePolicy On Pediatric Dental Pain ManagementمعتزباللهNessuna valutazione finora
- Drug StudyDocumento5 pagineDrug StudySarie LevitaNessuna valutazione finora
- Syiva Auliya Anjani (Critical Appraisal) JurnalDocumento11 pagineSyiva Auliya Anjani (Critical Appraisal) JurnalRagil SaputroNessuna valutazione finora
- Pneumonia FinalDocumento2 paginePneumonia FinalMMW MNessuna valutazione finora
- Nursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For InfluenzaDocumento6 pagineNursing Diagnosis Nursing Intervention Rationale: Prioritized Nursing Problem For InfluenzaJinaan MahmudNessuna valutazione finora
- Acupuncture Acupressure Shiatsu and ReflexologyDocumento46 pagineAcupuncture Acupressure Shiatsu and Reflexologyशशांक शेखर शुल्बNessuna valutazione finora
- The 10 Most Addictive Pain MedicationsDocumento17 pagineThe 10 Most Addictive Pain MedicationslabendetNessuna valutazione finora
- Pedo Seminar - Analgesics and Antibiotics Used in ChildrenDocumento44 paginePedo Seminar - Analgesics and Antibiotics Used in ChildrenPuneet ChoudharyNessuna valutazione finora
- Role of Vitamin BDocumento51 pagineRole of Vitamin BAnak Agung Indah PermatasariNessuna valutazione finora
- Dexmedetomidine ThesisDocumento7 pagineDexmedetomidine Thesisgingerschifflifortwayne100% (1)
- Bechet SindromDocumento10 pagineBechet SindromMarcel DocNessuna valutazione finora
- Enhanced Recovery After Surgery Protocols Decrease.12Documento7 pagineEnhanced Recovery After Surgery Protocols Decrease.12Ana BegovacNessuna valutazione finora
- Osteoarthritis Malaysian CPG 2013Documento25 pagineOsteoarthritis Malaysian CPG 2013aideeh3110100% (1)
- 100 Most Important DrugsDocumento13 pagine100 Most Important Drugsngopya djiki67% (3)
- Sma18 4742Documento24 pagineSma18 4742WDIV/ClickOnDetroitNessuna valutazione finora
- Sedación Consenso Alemania 2018 PDFDocumento76 pagineSedación Consenso Alemania 2018 PDFAnnison Hector Ramos BravoNessuna valutazione finora
- 2 in 1 P5VS Guideline 2018 (3rd Ed.) PDFDocumento50 pagine2 in 1 P5VS Guideline 2018 (3rd Ed.) PDFAzian ZainalNessuna valutazione finora
- Drug Study: Mechanis M OF ActionDocumento9 pagineDrug Study: Mechanis M OF ActionLovely San SebastianNessuna valutazione finora
- Balancing Method MirroringDocumento9 pagineBalancing Method MirroringYoshua ViventiusNessuna valutazione finora