Potrebbero piacerti anche
- Process Engineering ChiyodaDocumento65 pagineProcess Engineering ChiyodaSean Choi100% (10)
- Operation and MaintenanceDocumento41 pagineOperation and Maintenancegajendrabanshiwal8905100% (2)
- Operation and MaintenanceDocumento41 pagineOperation and Maintenancegajendrabanshiwal8905100% (2)
- LC Draft - InlandDocumento3 pagineLC Draft - Inlandgajendrabanshiwal8905100% (2)
- ExcavationDocumento18 pagineExcavationBogdan-Gabriel SchiopuNessuna valutazione finora
- CC Application PDF 221210050852Documento7 pagineCC Application PDF 221210050852Vishwas SalveNessuna valutazione finora
- Monotech GST Regg. UpDocumento3 pagineMonotech GST Regg. UpMONOTECH ACCOUNTSNessuna valutazione finora
- GST CertificateDocumento3 pagineGST CertificateNitin BirlaNessuna valutazione finora
- ZHI GST Certificate U.P.Documento3 pagineZHI GST Certificate U.P.Ansh RajanNessuna valutazione finora
- BRKCCT-1002 Cisco Live Contact CenterDocumento44 pagineBRKCCT-1002 Cisco Live Contact CenterArun GuptaNessuna valutazione finora
- Form GST REG-06: Government of IndiaDocumento3 pagineForm GST REG-06: Government of IndiaAishwary JainNessuna valutazione finora
- 6802988C45 ADocumento26 pagine6802988C45 AJose Luis Pardo FigueroaNessuna valutazione finora
- Form GST REG-06: Government of IndiaDocumento3 pagineForm GST REG-06: Government of IndiaRajendra JoshiNessuna valutazione finora
- Cobit 2019 Design Toolkit With Description - Group x.20201130165617871Documento46 pagineCobit 2019 Design Toolkit With Description - Group x.20201130165617871Izha Mahendra75% (4)
- Template For Table of Contents of RPMS PortfolioDocumento4 pagineTemplate For Table of Contents of RPMS PortfolioGener Toledo100% (4)
- (If Different From Registered Address) : Contact Details - SalesDocumento1 pagina(If Different From Registered Address) : Contact Details - Salesgajendrabanshiwal8905Nessuna valutazione finora
- Subscriber Registration FormDocumento6 pagineSubscriber Registration FormBhavin PatelNessuna valutazione finora
- Subscriber Registration FormDocumento6 pagineSubscriber Registration FormShorya moyalNessuna valutazione finora
- Nps S1FormDocumento6 pagineNps S1FormPOORNIMA GuptaNessuna valutazione finora
- National Pension System (Enps) - Subscriber Registration FormDocumento6 pagineNational Pension System (Enps) - Subscriber Registration Formajitp123Nessuna valutazione finora
- Subscriber Registration FormDocumento8 pagineSubscriber Registration Formvaristha upadhyay sanskrit SchoolNessuna valutazione finora
- Subscriber Registration FormDocumento6 pagineSubscriber Registration FormRahul PanwarNessuna valutazione finora
- Ilovepdf Merged PDFDocumento6 pagineIlovepdf Merged PDFPratham ModhaNessuna valutazione finora
- Application FormDocumento5 pagineApplication Formarshad1681987Nessuna valutazione finora
- Tata Memorial HospitalDocumento3 pagineTata Memorial Hospitalsiddhesh yewaleNessuna valutazione finora
- Odisha Police Recruitment Portal: Application For Engagement of Driver in PMT 2020Documento2 pagineOdisha Police Recruitment Portal: Application For Engagement of Driver in PMT 2020Sangram mohantyNessuna valutazione finora
- National Pension System (Enps) - Subscriber Registration FormDocumento7 pagineNational Pension System (Enps) - Subscriber Registration FormDRDA DHANBADNessuna valutazione finora
- Application FormDocumento5 pagineApplication FormMohit SharmaNessuna valutazione finora
- 06112015032845agreement VSNDocumento10 pagine06112015032845agreement VSNVISHESHNessuna valutazione finora
- CC Application PDF 230308083626Documento7 pagineCC Application PDF 230308083626JD GamingNessuna valutazione finora
- Application FormDocumento5 pagineApplication Formarjun trivediNessuna valutazione finora
- Indobright Services PVT LTD GST @Documento3 pagineIndobright Services PVT LTD GST @Ganesh RasankarNessuna valutazione finora
- Aa090224165982y RC27022024Documento3 pagineAa090224165982y RC27022024raj5487rajNessuna valutazione finora
- ApplicationDocumento5 pagineApplicationAkula Gopi KrishnaNessuna valutazione finora
- eNPSGDSFormDocumento3 pagineeNPSGDSFormAckee TechNessuna valutazione finora
- IB ACIO-II - Exe 2023Documento4 pagineIB ACIO-II - Exe 2023mohdshadabNessuna valutazione finora
- CC Application PDF 231028083450Documento8 pagineCC Application PDF 231028083450husainsk615Nessuna valutazione finora
- Vendor Registration FormDocumento3 pagineVendor Registration FormSourabh ShrivastavaNessuna valutazione finora
- Application FormDocumento5 pagineApplication FormVikas KumarNessuna valutazione finora
- GST K S Pulp CreatorsDocumento3 pagineGST K S Pulp Creatorsatul guptaNessuna valutazione finora
- (See Rule - ) Registration Certificate Issued Under SectionDocumento4 pagine(See Rule - ) Registration Certificate Issued Under SectionAnonymous gabKypRNessuna valutazione finora
- GST UpDocumento3 pagineGST UpAMAYRADH INFOTECHNessuna valutazione finora
- CVL and Ind Stocks Indmoney EsignDocumento92 pagineCVL and Ind Stocks Indmoney Esignnaman porwalNessuna valutazione finora
- National Pension System (Enps) - Subscriber Registration FormDocumento8 pagineNational Pension System (Enps) - Subscriber Registration FormSasankNessuna valutazione finora
- 5ybwsu - CMR - 1208180102308261 - 19 05 2022 16 16 23 638Documento1 pagina5ybwsu - CMR - 1208180102308261 - 19 05 2022 16 16 23 638harkeshNessuna valutazione finora
- Mandatory Fields Only For SV's From Assam and Meghalaya, Not Having Aadhaar Number # Data Fetching From AadhaarDocumento3 pagineMandatory Fields Only For SV's From Assam and Meghalaya, Not Having Aadhaar Number # Data Fetching From Aadhaarkeshav patelNessuna valutazione finora
- Application Form IciciDocumento5 pagineApplication Form IciciEsuresh5454Nessuna valutazione finora
- Application Form IciciDocumento5 pagineApplication Form IciciEsuresh5454Nessuna valutazione finora
- Sunshine Tower, 30 Floor, Senapati Bapat Marg, Dadar (West), MUMBAI, INDIA-400013 Phone - 022-61309999Documento1 paginaSunshine Tower, 30 Floor, Senapati Bapat Marg, Dadar (West), MUMBAI, INDIA-400013 Phone - 022-61309999Logesh Waran KmlNessuna valutazione finora
- Aa2002240191136 RC01032024Documento3 pagineAa2002240191136 RC01032024anzark84Nessuna valutazione finora
- PMS07200261456 LoanApplicationDocumento3 paginePMS07200261456 LoanApplicationbasantlodhi326Nessuna valutazione finora
- Application FormDocumento5 pagineApplication FormJagadeesh SuraNessuna valutazione finora
- GST Form-6 Dky Sales UP-1Documento3 pagineGST Form-6 Dky Sales UP-1suraj.kalambateNessuna valutazione finora
- RN009002 (Replica) AkkiDocumento5 pagineRN009002 (Replica) Akkiakshaykhairmode007Nessuna valutazione finora
- FRRO Appication FormDocumento3 pagineFRRO Appication FormHrishikesh Narasimhan100% (2)
- CMR 4xam8v SignDocumento1 paginaCMR 4xam8v SignSunita JaiswalNessuna valutazione finora
- Dznpk3427a 08dps9u 444608 1Documento1 paginaDznpk3427a 08dps9u 444608 1NAZEEF KHANNessuna valutazione finora
- Aa3702240087857 RC13022024Documento3 pagineAa3702240087857 RC13022024jptnetNessuna valutazione finora
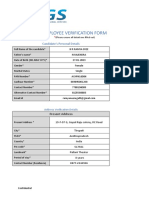
- Employee Verification Form - Ramya SreeDocumento4 pagineEmployee Verification Form - Ramya SreeRamyaNessuna valutazione finora
- Manoj Automobiles - GST CertificateDocumento3 pagineManoj Automobiles - GST Certificatewevaba5480Nessuna valutazione finora
- Union Bank of India (Tarnaka) : Signature Not VerifiedDocumento6 pagineUnion Bank of India (Tarnaka) : Signature Not VerifiedAnil AsangiNessuna valutazione finora
- Application FormDocumento5 pagineApplication Formabhijittathe18Nessuna valutazione finora
- Print - Udyam Registration Certificate1Documento2 paginePrint - Udyam Registration Certificate1caservice4allNessuna valutazione finora
- Aa0903240544862 RC14032024Documento3 pagineAa0903240544862 RC14032024ca.abhinavjain1Nessuna valutazione finora
- Shri Narayan Enterprises RCDocumento3 pagineShri Narayan Enterprises RCvanshcis014Nessuna valutazione finora
- View Generated DocsDocumento2 pagineView Generated DocsManuj RathoreNessuna valutazione finora
- Aa270323029027j RC15032023Documento3 pagineAa270323029027j RC15032023deepakjhaNessuna valutazione finora
- TALDocumento2 pagineTALSimran RoyNessuna valutazione finora
- Amc Letter (1227) JdaDocumento1 paginaAmc Letter (1227) Jdagajendrabanshiwal8905Nessuna valutazione finora
- Acceptance of ElevatorDocumento1 paginaAcceptance of Elevatorgajendrabanshiwal8905Nessuna valutazione finora
- Mile Stone Tracker - Royal HeritageDocumento2 pagineMile Stone Tracker - Royal Heritagegajendrabanshiwal8905Nessuna valutazione finora
- Tax Invoice: Thyssenkrupp Elevator (India) Pvt. LTDDocumento1 paginaTax Invoice: Thyssenkrupp Elevator (India) Pvt. LTDgajendrabanshiwal8905Nessuna valutazione finora
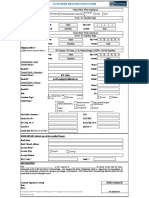
- Date of Material Delivery: ACO (800) ACO (800) Full Shipment Partial ShipmentDocumento3 pagineDate of Material Delivery: ACO (800) ACO (800) Full Shipment Partial Shipmentgajendrabanshiwal8905Nessuna valutazione finora
- 3 RD Party, Ganpati EnclaveDocumento2 pagine3 RD Party, Ganpati Enclavegajendrabanshiwal8905Nessuna valutazione finora
- Ho 20905025 26 27 28Documento1 paginaHo 20905025 26 27 28gajendrabanshiwal8905Nessuna valutazione finora
- Ho 20905007Documento1 paginaHo 20905007gajendrabanshiwal8905Nessuna valutazione finora
- 3 RD Party, City PlazaDocumento2 pagine3 RD Party, City Plazagajendrabanshiwal8905Nessuna valutazione finora
- Acceptance of ElevatorDocumento1 paginaAcceptance of Elevatorgajendrabanshiwal8905Nessuna valutazione finora
- Acceptance of ElevatorDocumento1 paginaAcceptance of Elevatorgajendrabanshiwal8905Nessuna valutazione finora
- Te MRLDocumento1 paginaTe MRLgajendrabanshiwal8905Nessuna valutazione finora
- Ho 005Documento1 paginaHo 005gajendrabanshiwal8905Nessuna valutazione finora
- Elavator Spare Parts, Elevator Cabins, Panels, Doors, Machinery Etc.Documento4 pagineElavator Spare Parts, Elevator Cabins, Panels, Doors, Machinery Etc.gajendrabanshiwal8905Nessuna valutazione finora
- The Cable System: Electric MotorDocumento4 pagineThe Cable System: Electric Motorgajendrabanshiwal8905Nessuna valutazione finora
- Ho 20905001Documento1 paginaHo 20905001gajendrabanshiwal8905Nessuna valutazione finora
- Ho 20904009Documento1 paginaHo 20904009gajendrabanshiwal8905Nessuna valutazione finora
- Terms and ConditionsDocumento8 pagineTerms and Conditionsgajendrabanshiwal8905Nessuna valutazione finora
- Material Supplers SAI MAKERSDocumento2 pagineMaterial Supplers SAI MAKERSgajendrabanshiwal8905Nessuna valutazione finora
- Car Operating Panels: For Front Return PanelDocumento12 pagineCar Operating Panels: For Front Return Panelgajendrabanshiwal8905Nessuna valutazione finora
- Market AreaDocumento1 paginaMarket Areagajendrabanshiwal8905Nessuna valutazione finora
- Elevator Gear Box: Special FeaturesDocumento2 pagineElevator Gear Box: Special Featuresgajendrabanshiwal8905Nessuna valutazione finora
- Te GLDocumento1 paginaTe GLgajendrabanshiwal8905Nessuna valutazione finora
- ECSS E ST 50 03C (31july2008)Documento43 pagineECSS E ST 50 03C (31july2008)jsadachiNessuna valutazione finora
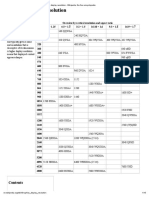
- Graphics Display Resolution - Wikipedia, The Free EncyclopediaDocumento15 pagineGraphics Display Resolution - Wikipedia, The Free EncyclopediaKarun KumarNessuna valutazione finora
- Rcfe Contract SSHDocumento240 pagineRcfe Contract SSHJeanne MarshNessuna valutazione finora
- ERJ 145 InfoDocumento11 pagineERJ 145 InfoMarcus100% (1)
- Comparison Between Six-Stroke and Four-Stroke EngineDocumento15 pagineComparison Between Six-Stroke and Four-Stroke EnginefaizanbasharatNessuna valutazione finora
- Xenon Xenalight Surgical Lighting SystemsDocumento2 pagineXenon Xenalight Surgical Lighting SystemsQasim AliNessuna valutazione finora
- 800ma Low Dropout Positive Regulator: Features DescriptionDocumento12 pagine800ma Low Dropout Positive Regulator: Features DescriptionmarcianocalviNessuna valutazione finora
- SBI Clerk Mains Bolt 2023 OliveboardDocumento160 pagineSBI Clerk Mains Bolt 2023 OliveboardMaahi ThakorNessuna valutazione finora
- 11kv BB1Documento1 pagina11kv BB1Hammadiqbal12Nessuna valutazione finora
- Bluetooth: Short Range Wireless Connectivity StandardDocumento10 pagineBluetooth: Short Range Wireless Connectivity StandardSorceress5Nessuna valutazione finora
- Whose Online Video Lectures Are Best For The IIT JEE?Documento6 pagineWhose Online Video Lectures Are Best For The IIT JEE?Buzz PriyanshuNessuna valutazione finora
- DH Xvr4b16Documento3 pagineDH Xvr4b16Jumar JumadiaoNessuna valutazione finora
- Is 13687 1993Documento15 pagineIs 13687 1993ADIPESHNessuna valutazione finora
- White Products CatalogDocumento49 pagineWhite Products CatalogjesusNessuna valutazione finora
- Bloomberg Certification FAQ BMC (Bloomberg Market Concepts) : Goizueta Business LibraryDocumento3 pagineBloomberg Certification FAQ BMC (Bloomberg Market Concepts) : Goizueta Business LibrarySarah Raquel Bozo Herrera100% (1)
- Boomer M-Series Technical Specification tcm835-1533266 PDFDocumento8 pagineBoomer M-Series Technical Specification tcm835-1533266 PDFseferinoNessuna valutazione finora
- The Impact of Greed On Academic Medicine and Patient CareDocumento5 pagineThe Impact of Greed On Academic Medicine and Patient CareBhawana Prashant AgrawalNessuna valutazione finora
- PESTLE Analysis Patanjali Ayurved LTDDocumento7 paginePESTLE Analysis Patanjali Ayurved LTDvaidehi50% (2)
- Getting Started With ATV310: DangerDocumento4 pagineGetting Started With ATV310: DangerAdnan Naeem MalikNessuna valutazione finora
- Analyzing and Securing Social Media: Cloud-Based Assured Information SharingDocumento36 pagineAnalyzing and Securing Social Media: Cloud-Based Assured Information SharingakrmbaNessuna valutazione finora
- Jinko 570 Mono Facial Jkm570m-7rl4-VDocumento2 pagineJinko 570 Mono Facial Jkm570m-7rl4-VShahneela AnsariNessuna valutazione finora
- 7ML19981GC61 1Documento59 pagine7ML19981GC61 1Andres ColladoNessuna valutazione finora
- Case StudyDocumento80 pagineCase Studybravo deltafoxNessuna valutazione finora
- H S ™ PHC P H C: Ypertherm Ensor Lasma Eight OntrolDocumento58 pagineH S ™ PHC P H C: Ypertherm Ensor Lasma Eight OntrolCRISTIANNessuna valutazione finora