Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- 1 PBDocumento13 pagine1 PBstefany huangNessuna valutazione finora
- Personality Disorder and Management Block 2.4: Carla R MarchiraDocumento38 paginePersonality Disorder and Management Block 2.4: Carla R MarchiraadystiNessuna valutazione finora
- Lecture 6.5 Fracture and Dislocation-Dr. Yudha Mathan Sakti, SP - Ot (K) (2020)Documento81 pagineLecture 6.5 Fracture and Dislocation-Dr. Yudha Mathan Sakti, SP - Ot (K) (2020)stefany huangNessuna valutazione finora
- Lecture 24-Symptomatology in Psychiatry in Correlation With Mental Disorder-Dr. Irwan Supriyanto, SP - KJ, Ph.D. (2019)Documento22 pagineLecture 24-Symptomatology in Psychiatry in Correlation With Mental Disorder-Dr. Irwan Supriyanto, SP - KJ, Ph.D. (2019)stefany huangNessuna valutazione finora
- Lecture 2.5 Eyes Injuries-Dr. Purjanto Tepo Utomo, SP.M (K) (2020)Documento34 pagineLecture 2.5 Eyes Injuries-Dr. Purjanto Tepo Utomo, SP.M (K) (2020)stefany huangNessuna valutazione finora
- Knowledge Attitude and Behaviour of Patients TowarDocumento5 pagineKnowledge Attitude and Behaviour of Patients Towarstefany huangNessuna valutazione finora
- Sce 1Documento1 paginaSce 1stefany huangNessuna valutazione finora
- Slide Ajar B.1 (Asdos 14)Documento102 pagineSlide Ajar B.1 (Asdos 14)stefany huangNessuna valutazione finora
- Lecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)Documento63 pagineLecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)stefany huangNessuna valutazione finora
- Slide Ajar B.1 (Asdos 14)Documento102 pagineSlide Ajar B.1 (Asdos 14)stefany huangNessuna valutazione finora
- Lecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)Documento63 pagineLecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)stefany huangNessuna valutazione finora
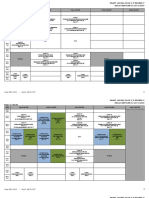
- Jadwal C.5 Reg - FinalDocumento6 pagineJadwal C.5 Reg - Finalstefany huangNessuna valutazione finora
- Lecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFDocumento37 pagineLecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFstefany huangNessuna valutazione finora
- DHF Menurut WHO 2011Documento212 pagineDHF Menurut WHO 2011Jamal SutrisnaNessuna valutazione finora
- Lecture 26-Skin Cancer-Dr. Dr. Y. Widodo Wirohadidjojo, SP - KK (K) (2020)Documento43 pagineLecture 26-Skin Cancer-Dr. Dr. Y. Widodo Wirohadidjojo, SP - KK (K) (2020)stefany huangNessuna valutazione finora
- Introduction To Surgical OncologyDocumento39 pagineIntroduction To Surgical OncologyLestariIrawanHadiNessuna valutazione finora
- Lecture 31-Tourette Disorder Tics-Dr. Mahar Agusno, SP - KJ. (K) - (2020)Documento12 pagineLecture 31-Tourette Disorder Tics-Dr. Mahar Agusno, SP - KJ. (K) - (2020)stefany huangNessuna valutazione finora
- Lecture 25-Neoplastic and Non-Neoplastic Diseases in Genitourinary System of The Elderly-Dr. Danarto, SP.B., Sp.U (2020)Documento38 pagineLecture 25-Neoplastic and Non-Neoplastic Diseases in Genitourinary System of The Elderly-Dr. Danarto, SP.B., Sp.U (2020)stefany huangNessuna valutazione finora
- Jadwal C.5 Reg - FinalDocumento6 pagineJadwal C.5 Reg - Finalstefany huangNessuna valutazione finora
- Lecture 36-Hormonal and Metabolism Disorder-Dr. Vina Yanti S., M.SC., SP - PD., PH.D (2020)Documento24 pagineLecture 36-Hormonal and Metabolism Disorder-Dr. Vina Yanti S., M.SC., SP - PD., PH.D (2020)stefany huangNessuna valutazione finora
- Lecture 14-Infectious Diseases and Sepsis in Elderly-Dr. Rizka Humardewayanti A, SP - PD-KPTI (2019)Documento89 pagineLecture 14-Infectious Diseases and Sepsis in Elderly-Dr. Rizka Humardewayanti A, SP - PD-KPTI (2019)stefany huangNessuna valutazione finora
- Lecture 13-Immunodefficiency in Elderly-Dr. Eko Aribowo, M.Kes, SpPD-KGer (2019)Documento30 pagineLecture 13-Immunodefficiency in Elderly-Dr. Eko Aribowo, M.Kes, SpPD-KGer (2019)stefany huangNessuna valutazione finora
- Anatomy of Blood Vessels and Lymphatics-Santosa Budiharjo (2016)Documento46 pagineAnatomy of Blood Vessels and Lymphatics-Santosa Budiharjo (2016)stefany huangNessuna valutazione finora
- Lecture 27-Principles of Chemotherapy-Dr. Ibnu Purwanto, SP - PD., KHOM (2020)Documento56 pagineLecture 27-Principles of Chemotherapy-Dr. Ibnu Purwanto, SP - PD., KHOM (2020)stefany huangNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Mindfulness and Acceptance For Addictive Behaviors Applying Contextual CBT To Substance Abuse and Behavioral AddictionsDocumento354 pagineMindfulness and Acceptance For Addictive Behaviors Applying Contextual CBT To Substance Abuse and Behavioral AddictionsAlejandra Vergara83% (6)
- Psychedelic Substances: The Little Book ofDocumento46 paginePsychedelic Substances: The Little Book ofpepe100% (2)
- Nursing Management of Patients With Occupational DisordersDocumento100 pagineNursing Management of Patients With Occupational DisordersNandini VermaNessuna valutazione finora
- Healthcare Analytical Testing ServicesDocumento34 pagineHealthcare Analytical Testing ServicesAaryan AgrahariNessuna valutazione finora
- Cystic Fibrosis: SymptomsDocumento2 pagineCystic Fibrosis: SymptomsMehrul Singh RanavatNessuna valutazione finora
- Referat Sudden Death - ForensikDocumento44 pagineReferat Sudden Death - ForensikMuhamad PascadhNessuna valutazione finora
- DLL in MAPEH 6 - Health Week 10Documento4 pagineDLL in MAPEH 6 - Health Week 10Sara Jane C. Jose-TayaoNessuna valutazione finora
- Disaster Management at Site and at HospitalDocumento21 pagineDisaster Management at Site and at HospitalAlmasNessuna valutazione finora
- TLE 7 Health and Safety in The KItchenDocumento32 pagineTLE 7 Health and Safety in The KItchenChristine Mabelle AlmojuelaNessuna valutazione finora
- Jurnal CoklatDocumento16 pagineJurnal CoklatRoby martinus bayaNessuna valutazione finora
- Family PlanningDocumento15 pagineFamily PlanningOkky isNessuna valutazione finora
- Abrams Clinical Drug Therapy 10th Edition Frandsen Test BankDocumento25 pagineAbrams Clinical Drug Therapy 10th Edition Frandsen Test BankMissKatherineGardnerfjcp100% (46)
- Performance Belgian Health SystemDocumento117 paginePerformance Belgian Health SystemM Faozi KurniawanNessuna valutazione finora
- Safety Data Sheet: K-37 Septic Tank Treatment 1. Product Identification K-37 Septic Tank TreatmentDocumento7 pagineSafety Data Sheet: K-37 Septic Tank Treatment 1. Product Identification K-37 Septic Tank TreatmentRicardo AlvaradoNessuna valutazione finora
- 01 Conference Nursing 2023 - Tentative Program - R2Documento1 pagina01 Conference Nursing 2023 - Tentative Program - R2Nurul syakinah Binti mohd mohidNessuna valutazione finora
- CV UPDATE Agt, 2021Documento6 pagineCV UPDATE Agt, 2021nadita erischaNessuna valutazione finora
- Meniere's DiseaseDocumento46 pagineMeniere's Diseaseabhinay_1712Nessuna valutazione finora
- PCORI Methodology Standards Curriculum Research Questions 3Documento13 paginePCORI Methodology Standards Curriculum Research Questions 3Krizele Acu PagalananNessuna valutazione finora
- Students Health SurveyDocumento1 paginaStudents Health SurveyJulie Basbas-CruzNessuna valutazione finora
- Medical Services Division: Hi-Precision Diagnostics (V Luna Branch)Documento1 paginaMedical Services Division: Hi-Precision Diagnostics (V Luna Branch)Ren RenNessuna valutazione finora
- Pre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MDocumento55 paginePre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MBini JaminNessuna valutazione finora
- Registration at AWC-EnglishDocumento2 pagineRegistration at AWC-EnglishSamtha MasineniNessuna valutazione finora
- Nursing ManagementDocumento24 pagineNursing ManagementSimran Josan100% (1)
- Diet HistoryDocumento2 pagineDiet HistoryBea Lou SabadoNessuna valutazione finora
- Clinical Practice Guidelines and ProtocolsDocumento4 pagineClinical Practice Guidelines and ProtocolsMahmoud NaggarNessuna valutazione finora
- Unit VI L&D Case StudyDocumento6 pagineUnit VI L&D Case StudyBrooke Misty Ann BaileyNessuna valutazione finora
- Fourth Grading NotesDocumento70 pagineFourth Grading NotesMini RinnNessuna valutazione finora
- Avendus Live ProjectDocumento2 pagineAvendus Live ProjectRishabh GuptaNessuna valutazione finora
- Research PaperDocumento28 pagineResearch PaperMarcelNessuna valutazione finora
- Outcomes For The Early Learning FrameworkDocumento6 pagineOutcomes For The Early Learning Frameworkapi-319447682100% (1)