Potrebbero piacerti anche
- Manjunath - Metabical-Positioning & Communication StrategyDocumento3 pagineManjunath - Metabical-Positioning & Communication Strategynmanj0% (1)
- Justice League UnlimitedDocumento22 pagineJustice League UnlimitedCrystel Tze Jing100% (5)
- How To Write A Lab Report For MUFY Biology Units 1 and 2 (2014)Documento25 pagineHow To Write A Lab Report For MUFY Biology Units 1 and 2 (2014)Crystel Tze JingNessuna valutazione finora
- Isorobik AdDocumento2 pagineIsorobik AdaghorbanzadehNessuna valutazione finora
- Some Sampling Distribution ProblemsDocumento3 pagineSome Sampling Distribution ProblemsvuduyducNessuna valutazione finora
- Excerpt: "Fat Chance" by Robert LustigDocumento3 pagineExcerpt: "Fat Chance" by Robert Lustigwamu885067% (3)
- Insulin and Oral Hypoglycemic AgentsDocumento27 pagineInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)
- Antidiabetic Drug PDFDocumento91 pagineAntidiabetic Drug PDFAlifia ainushNessuna valutazione finora
- Treatment of Diabetes MellitusDocumento31 pagineTreatment of Diabetes MellitusIrfan IdealistNessuna valutazione finora
- A Practical Guide To Insulin TherapyDocumento42 pagineA Practical Guide To Insulin Therapyseun williams100% (2)
- Terapi Insulin-1Documento46 pagineTerapi Insulin-1Yanti MoonNessuna valutazione finora
- Pharmacotherapy of Alzheimers DiseaseDocumento69 paginePharmacotherapy of Alzheimers DiseaseCAROL ANN PATITICONessuna valutazione finora
- Subutex Quick-Start-GuideDocumento6 pagineSubutex Quick-Start-GuideDanNessuna valutazione finora
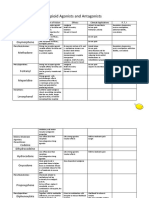
- Opioid Agonists and AntagonistsDocumento5 pagineOpioid Agonists and AntagonistsCas BuNessuna valutazione finora
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocumento69 paginePancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNessuna valutazione finora
- Management of DyslipidemiaDocumento35 pagineManagement of DyslipidemiaAmir MahmoudNessuna valutazione finora
- Critical Care Drugs 1Documento21 pagineCritical Care Drugs 1Asri ErnadiNessuna valutazione finora
- Substance-Related and Addictive Disorders (Presentation)Documento219 pagineSubstance-Related and Addictive Disorders (Presentation)Ryan Wong [Aizen]Nessuna valutazione finora
- Case Study For Di 1Documento14 pagineCase Study For Di 1api-515538459Nessuna valutazione finora
- Diabetes ValuesDocumento67 pagineDiabetes Valuesluckytung07100% (1)
- Oleander PoisoningDocumento19 pagineOleander PoisoningAnbu Arasan100% (1)
- How To Administer InsulinDocumento2 pagineHow To Administer Insulinapi-375248140Nessuna valutazione finora
- Vivitrol TreatmentDocumento8 pagineVivitrol TreatmentHarish RathodNessuna valutazione finora
- Insulin Types: According To Mode of Action: Rapid Acting Insulin Intermediate Acting Insulin Biphasic InsulinsDocumento1 paginaInsulin Types: According To Mode of Action: Rapid Acting Insulin Intermediate Acting Insulin Biphasic InsulinsAssem Ashraf Khidhr100% (1)
- Insulin Initiation PPT - PPTX 2Documento53 pagineInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Insulin HandbookDocumento67 pagineInsulin HandbookThits SarNessuna valutazione finora
- Dosage CalculationsDocumento21 pagineDosage CalculationsHaley P100% (2)
- ROYAL COLLEGE - Diabetic Ketoacidosis. Update On ManagementDocumento3 pagineROYAL COLLEGE - Diabetic Ketoacidosis. Update On ManagementFatos KatanolliNessuna valutazione finora
- 3a Emergency Care DKA (UK) FINALDocumento40 pagine3a Emergency Care DKA (UK) FINALDrsarfaraz SiddiquiNessuna valutazione finora
- ( (Drugs For Diabetes Mellitus) ) PDFDocumento7 pagine( (Drugs For Diabetes Mellitus) ) PDFMohamedYosefNessuna valutazione finora
- Insulin Injection Tutorial ExmDocumento13 pagineInsulin Injection Tutorial ExmAslah NabilahNessuna valutazione finora
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDocumento34 pagineHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyasNessuna valutazione finora
- Dka CalculatorDocumento1 paginaDka CalculatorTalib AdilNessuna valutazione finora
- Diabetes Mellitus: Dr. Sajid Abbas JaffriDocumento37 pagineDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinNessuna valutazione finora
- Impactednurse Nurses Reference PackDocumento2 pagineImpactednurse Nurses Reference PackRaenell CurryNessuna valutazione finora
- Drugs in ObstetricsDocumento95 pagineDrugs in ObstetricsPriya jNessuna valutazione finora
- Diabetes: Causes, Symptoms and TreatmentsDocumento4 pagineDiabetes: Causes, Symptoms and TreatmentsAbdullah BazryNessuna valutazione finora
- Case StudyDocumento6 pagineCase Studyapi-276551783Nessuna valutazione finora
- Approach To A Non-Resolving PnemoniaDocumento20 pagineApproach To A Non-Resolving PnemoniaFelix ManyerukeNessuna valutazione finora
- Insulin and Anti Diabetic DrugsDocumento38 pagineInsulin and Anti Diabetic DrugsDharun Ranganathan100% (1)
- Acute Complications of Diabetes MellitusDocumento43 pagineAcute Complications of Diabetes MellitusalphaphoenixNessuna valutazione finora
- A Guide To ECG Reporting For Year 3 Medical StudentsDocumento2 pagineA Guide To ECG Reporting For Year 3 Medical StudentscsngiuNessuna valutazione finora
- Med Admin Practice QuestionsDocumento5 pagineMed Admin Practice QuestionsArmelle DelvaNessuna valutazione finora
- Galectin ReviewDocumento24 pagineGalectin ReviewmaniiiiiiiiNessuna valutazione finora
- DKA Canadian ProtocolDocumento2 pagineDKA Canadian Protocolplay_wright2084Nessuna valutazione finora
- DyslipidemiaDocumento18 pagineDyslipidemiaDeepthi Avvaru100% (1)
- Practical Guidance On The Use of Premix Insulin - FinalDocumento14 paginePractical Guidance On The Use of Premix Insulin - FinalJonesius Eden ManoppoNessuna valutazione finora
- Uterine RelaxantsDocumento17 pagineUterine RelaxantsSharad BhallaNessuna valutazione finora
- Diabetic KetoacidosisDocumento27 pagineDiabetic Ketoacidosisjun sianNessuna valutazione finora
- Guideline Methadone MaintenanceDocumento133 pagineGuideline Methadone MaintenancearthurmathieuNessuna valutazione finora
- Diabetic Ketoacidosis in Pregnancy: Diagnosis of DKADocumento7 pagineDiabetic Ketoacidosis in Pregnancy: Diagnosis of DKA123someone123Nessuna valutazione finora
- Anasthetic DrugsDocumento62 pagineAnasthetic DrugsMilda InayahNessuna valutazione finora
- 128 Diabetic KetoacidosisDocumento9 pagine128 Diabetic KetoacidosisDite Bayu NugrohoNessuna valutazione finora
- Ventricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmDocumento2 pagineVentricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmsafasayedNessuna valutazione finora
- Guidelines For Management of Diabetes MellitusDocumento1 paginaGuidelines For Management of Diabetes MellitusthapanNessuna valutazione finora
- Adrenergic AgonistsDocumento40 pagineAdrenergic AgonistsBenedict Brashi100% (1)
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocumento66 pagineDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManElvis J. DavisNessuna valutazione finora
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocumento1 paginaDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- DiabetesDocumento99 pagineDiabetes489226fahimNessuna valutazione finora
- Recent Trials in Neonatology - Part IIDocumento70 pagineRecent Trials in Neonatology - Part IIPranay MallNessuna valutazione finora
- Structured Patient Education Diabetes ReportDocumento76 pagineStructured Patient Education Diabetes ReportPatrick Commettant100% (1)
- PATIENT 1 Nursing Assessment FormDocumento5 paginePATIENT 1 Nursing Assessment FormndemboloveNessuna valutazione finora
- Case Note 20: Patient DetailsDocumento3 pagineCase Note 20: Patient DetailsBINCYNessuna valutazione finora
- Case Presentation CRUH FinalDocumento27 pagineCase Presentation CRUH FinalMatthew LeiNessuna valutazione finora
- Clinical Order Set DKA AdultDocumento2 pagineClinical Order Set DKA AdultBashar Al-HamaidehNessuna valutazione finora
- Pharmacology of Diabetes Mellitus: Glucose RegulationDocumento33 paginePharmacology of Diabetes Mellitus: Glucose RegulationAbdullah RawashdehNessuna valutazione finora
- BibleReadingSchedule2020 PDFDocumento2 pagineBibleReadingSchedule2020 PDFGabrielNessuna valutazione finora
- Pregnancy Induced Vomiting and Hyperemesis Gravidarum - CG2016Documento11 paginePregnancy Induced Vomiting and Hyperemesis Gravidarum - CG2016Crystel Tze JingNessuna valutazione finora
- Module 21 - Malaysia - Double Burden of MalnutritionDocumento8 pagineModule 21 - Malaysia - Double Burden of MalnutritionCrystel Tze JingNessuna valutazione finora
- Mechanism and Stages of LabourDocumento1 paginaMechanism and Stages of LabourCrystel Tze JingNessuna valutazione finora
- Disease Mechanism and Neoplasia RevisionDocumento5 pagineDisease Mechanism and Neoplasia RevisionCrystel Tze JingNessuna valutazione finora
- Liver RevisionDocumento61 pagineLiver RevisionCrystel Tze JingNessuna valutazione finora
- Evolution of Life 2014Documento40 pagineEvolution of Life 2014Crystel Tze JingNessuna valutazione finora
- Answers To 2010 PapersDocumento4 pagineAnswers To 2010 PapersCrystel Tze JingNessuna valutazione finora
- An Approach To Common Urological Disorders PDFDocumento45 pagineAn Approach To Common Urological Disorders PDFCrystel Tze JingNessuna valutazione finora
- Bio Lab ReportDocumento2 pagineBio Lab ReportCrystel Tze JingNessuna valutazione finora
- AestheticsAsia Congress Brochure PDFDocumento12 pagineAestheticsAsia Congress Brochure PDFCrystel Tze JingNessuna valutazione finora
- Mango Smoothie SurpriseDocumento3 pagineMango Smoothie SurpriseCrystel Tze JingNessuna valutazione finora
- Rotary Is Made Up of Three PartsDocumento3 pagineRotary Is Made Up of Three PartsCrystel Tze JingNessuna valutazione finora
- One M Sia Public SpeakingDocumento1 paginaOne M Sia Public SpeakingBlue ButterNessuna valutazione finora
- Rotary Is Made Up of Three PartsDocumento3 pagineRotary Is Made Up of Three PartsCrystel Tze JingNessuna valutazione finora
- 8pecomplete 140709171348 Phpapp01 PDFDocumento201 pagine8pecomplete 140709171348 Phpapp01 PDFJuliene De Los SantosNessuna valutazione finora
- Morning Report CKDDocumento20 pagineMorning Report CKDjoe joeNessuna valutazione finora
- Lazar Angelov Interview PDFDocumento13 pagineLazar Angelov Interview PDFVarun RanaNessuna valutazione finora
- NUT 116AL Obesity Case StudyDocumento10 pagineNUT 116AL Obesity Case StudyAkarin MittongtareNessuna valutazione finora
- Fitt Log Worksheet 5Documento2 pagineFitt Log Worksheet 5api-270355373Nessuna valutazione finora
- Latihan Soal UTS Kesetaraan Paket C Kelas 11Documento1 paginaLatihan Soal UTS Kesetaraan Paket C Kelas 11Novince F PuspitariaNessuna valutazione finora
- Finished CaliUnity LeafletDocumento2 pagineFinished CaliUnity LeafletOlllie OlllieNessuna valutazione finora
- Weightlifting Program DesignDocumento8 pagineWeightlifting Program DesignManish ShahNessuna valutazione finora
- PEH ReviewerDocumento2 paginePEH ReviewerKazuma TaikiNessuna valutazione finora
- Cardiovascular and CerebrovascularDocumento6 pagineCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- PoemDocumento8 paginePoemJeevitraNessuna valutazione finora
- Typology of Family Nursing Health CareDocumento9 pagineTypology of Family Nursing Health Careryujin babieNessuna valutazione finora
- Protein Energy MalnutritionDocumento30 pagineProtein Energy Malnutritionadeelyaseen1Nessuna valutazione finora
- B-MIDTERMS EXAM-NutriLECDocumento7 pagineB-MIDTERMS EXAM-NutriLECNelia AlfonsoNessuna valutazione finora
- Nutrition 409 - Case 12Documento2 pagineNutrition 409 - Case 12api-252471038Nessuna valutazione finora
- Macro CalculatorDocumento1 paginaMacro CalculatorJoul BitarNessuna valutazione finora
- Grade 1 Pattern of LV Diastolic FillingDocumento3 pagineGrade 1 Pattern of LV Diastolic FillingNicoleNessuna valutazione finora
- 10 Week Mass Building Program - HTML PDFDocumento19 pagine10 Week Mass Building Program - HTML PDFdoc moNessuna valutazione finora
- Obesity, Diets, and Social Inequalities PDFDocumento5 pagineObesity, Diets, and Social Inequalities PDFSalmiah OthmanNessuna valutazione finora
- Stunting (EDIT)Documento62 pagineStunting (EDIT)Eka RahmawatiNessuna valutazione finora
- CKD 2016Documento39 pagineCKD 2016husnaNessuna valutazione finora
- Efectos de Una Dieta Hipocalórica PDFDocumento6 pagineEfectos de Una Dieta Hipocalórica PDFGertru Vargas MolinaNessuna valutazione finora
- Diet and Activity Analysis PaperDocumento19 pagineDiet and Activity Analysis Paperapi-353042837Nessuna valutazione finora
- Oil Palm Fractions Derivatives Web PDFDocumento6 pagineOil Palm Fractions Derivatives Web PDFIan RidzuanNessuna valutazione finora
- DR Nowzaradan Diet PlanDocumento10 pagineDR Nowzaradan Diet PlanfightformotivationNessuna valutazione finora
- AA Protein EnzymeDocumento64 pagineAA Protein EnzymeNash DeniegaNessuna valutazione finora