Potrebbero piacerti anche
- Athraa A. Mahmood M.Sc. of Periodontics: Prepared byDocumento22 pagineAthraa A. Mahmood M.Sc. of Periodontics: Prepared byheycoolalexNessuna valutazione finora
- Mingival Curettage PDFDocumento52 pagineMingival Curettage PDFheycoolalexNessuna valutazione finora
- Midline Diastema PDFDocumento33 pagineMidline Diastema PDFheycoolalex100% (1)
- Connects Components To The Major Connector: Minor ConnectorsDocumento25 pagineConnects Components To The Major Connector: Minor ConnectorsheycoolalexNessuna valutazione finora
- Fixed ProsthodonticsDocumento13 pagineFixed ProsthodonticsheycoolalexNessuna valutazione finora
- Ergonomics in DentistryDocumento55 pagineErgonomics in DentistryheycoolalexNessuna valutazione finora
- Cranial Base Angle in Relation To MalocclusionDocumento50 pagineCranial Base Angle in Relation To Malocclusionheycoolalex100% (1)
- Articulators: Lek. Dent. Krzysztof Gawriołek Oral Rehabilitation ClinicDocumento36 pagineArticulators: Lek. Dent. Krzysztof Gawriołek Oral Rehabilitation ClinicheycoolalexNessuna valutazione finora
- Anatomy and Clinical Significance of Denture Bearing AreasDocumento60 pagineAnatomy and Clinical Significance of Denture Bearing AreasheycoolalexNessuna valutazione finora
- Bomechancs in OrthodotnicsDocumento74 pagineBomechancs in OrthodotnicsheycoolalexNessuna valutazione finora
- Ceramic Inlays Is The Inlay Thickness An Important Factor Influencing The Fracture RiskDocumento8 pagineCeramic Inlays Is The Inlay Thickness An Important Factor Influencing The Fracture RiskheycoolalexNessuna valutazione finora
- Conenctors in FPDDocumento18 pagineConenctors in FPDheycoolalexNessuna valutazione finora
- Abutment Selection in Fixed Partial Denture PDFDocumento6 pagineAbutment Selection in Fixed Partial Denture PDFheycoolalexNessuna valutazione finora
- Aberrant Frenum and Its TreatmentDocumento90 pagineAberrant Frenum and Its TreatmentheycoolalexNessuna valutazione finora
- Abutment Selection in Fixed Partial DentureDocumento6 pagineAbutment Selection in Fixed Partial DentureheycoolalexNessuna valutazione finora
- Four-Year Clinical Evaluation of A Self-Adhesive Luting Agent For Ceramic InlaysDocumento12 pagineFour-Year Clinical Evaluation of A Self-Adhesive Luting Agent For Ceramic InlaysheycoolalexNessuna valutazione finora
- BASELINE SETTINGS FOR DENTAL PHOTOGRAPHY (Schoenbaum - UCLA)Documento2 pagineBASELINE SETTINGS FOR DENTAL PHOTOGRAPHY (Schoenbaum - UCLA)heycoolalexNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Materi 2 - Cause Effect - SMA Kelas XIDocumento7 pagineMateri 2 - Cause Effect - SMA Kelas XIedrianNessuna valutazione finora
- Rulebook Newton PDFDocumento16 pagineRulebook Newton PDFvaggos1988Nessuna valutazione finora
- Unwedge Getting Started CompressedDocumento4 pagineUnwedge Getting Started CompressedJuan Carlos Rosas San AgustinNessuna valutazione finora
- Advanced Control Theory 2nd Nagoor KaniDocumento3 pagineAdvanced Control Theory 2nd Nagoor Kaniunnvishnu20% (25)
- Grade 11-Personal Development-Q1 Module 1Documento30 pagineGrade 11-Personal Development-Q1 Module 1nathaniel catbaganNessuna valutazione finora
- Rigid Pipeline DesignDocumento123 pagineRigid Pipeline DesignAditya Prasad100% (1)
- A Very Good Read On The Construction of Natural NumbersDocumento5 pagineA Very Good Read On The Construction of Natural NumbersBadd ManNessuna valutazione finora
- Dokumen - Tips - University Physics With Modern Physics 12th Edition Searched For A Ebook byDocumento7 pagineDokumen - Tips - University Physics With Modern Physics 12th Edition Searched For A Ebook byJuan FernándezNessuna valutazione finora
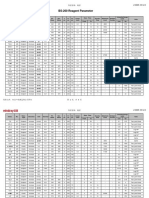
- BS-200 Reagent ParameterDocumento3 pagineBS-200 Reagent ParameterBetina NdjiemiNessuna valutazione finora
- MBEH'S - Final - Work (1) 27Documento72 pagineMBEH'S - Final - Work (1) 27Fon Palverd Brent BridenNessuna valutazione finora
- CompleteMaxwell3D V15Documento1.006 pagineCompleteMaxwell3D V15Truong Cong TrinhNessuna valutazione finora
- Assignment 1Documento2 pagineAssignment 1Nitish KumarNessuna valutazione finora
- Assignment - AER03630 3 2023Documento2 pagineAssignment - AER03630 3 2023BrandonNessuna valutazione finora
- m7 L8-Hydraulic Design of Sewers and Storm Water DrainageDocumento8 paginem7 L8-Hydraulic Design of Sewers and Storm Water DrainageEngr Asad SufyanNessuna valutazione finora
- Language Paper 1 - Q SDocumento8 pagineLanguage Paper 1 - Q Ssaumya.pardeshiNessuna valutazione finora
- SR2019-06 (RD) Atlas of Siliceous Hot Spring Deposits - FINALDocumento62 pagineSR2019-06 (RD) Atlas of Siliceous Hot Spring Deposits - FINALMichael Platas100% (1)
- 100-149 Bac 2010-2019Documento169 pagine100-149 Bac 2010-2019Maria RusschihNessuna valutazione finora
- Burning A Candle WorksheetDocumento3 pagineBurning A Candle Worksheetmahdibba670Nessuna valutazione finora
- Folleto GA1-240202501-AA2-EV01Documento2 pagineFolleto GA1-240202501-AA2-EV01Katherine Zapata33% (3)
- Unit 2Documento24 pagineUnit 2Milka RahmanNessuna valutazione finora
- OCR Physics A: 12.3 The Young Double-Slit Experiment Teacher and Technician NotesDocumento5 pagineOCR Physics A: 12.3 The Young Double-Slit Experiment Teacher and Technician NotessciencedocsmanNessuna valutazione finora
- Earthquak Analysis in AnsysDocumento14 pagineEarthquak Analysis in AnsysIgor GjorgjievNessuna valutazione finora
- Bio-Cultural and Political Evolution of ManDocumento18 pagineBio-Cultural and Political Evolution of ManKentarou SakaguchiNessuna valutazione finora
- Culture Communication and SilenceDocumento20 pagineCulture Communication and SilencerogarhiNessuna valutazione finora
- The Development of Coping Resources in Adulthood: Carolyn M. Aldwin and Karen J. SuttonDocumento36 pagineThe Development of Coping Resources in Adulthood: Carolyn M. Aldwin and Karen J. SuttonZuluaga LlanedNessuna valutazione finora
- Lucas Buchaillot 1ere3Documento2 pagineLucas Buchaillot 1ere3buchaillotlucas1Nessuna valutazione finora
- SKF Slim Thin BearingsDocumento139 pagineSKF Slim Thin Bearingsaghamdi2206Nessuna valutazione finora
- Hán Công Đỉnh 20195767Documento46 pagineHán Công Đỉnh 20195767Hán Công ĐỉnhNessuna valutazione finora
- SAMEEEEEEEEDocumento68 pagineSAMEEEEEEEEMarjorie MalvedaNessuna valutazione finora
- Winstar Display Co., LTD: SpecificationDocumento24 pagineWinstar Display Co., LTD: SpecificationElvis SilvaNessuna valutazione finora