Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- (Research Work) BS4S14-V1-21411 - O21411G20671 - Research Methods - R1704D2623249 - Osagie ObazeeDocumento21 pagine(Research Work) BS4S14-V1-21411 - O21411G20671 - Research Methods - R1704D2623249 - Osagie ObazeeKing KosherNessuna valutazione finora
- Safety/ Forms / Gen/Covid-19 G: Provisionary Canteen ChecklistDocumento5 pagineSafety/ Forms / Gen/Covid-19 G: Provisionary Canteen Checklistuttam mishraNessuna valutazione finora
- Narrative Essay About Covid 19Documento3 pagineNarrative Essay About Covid 19Leshwa Mendigroya100% (7)
- RRL 1Documento5 pagineRRL 1Boy MadNessuna valutazione finora
- Coronavirus: Say True or False Answer The Following QuestionsDocumento1 paginaCoronavirus: Say True or False Answer The Following QuestionsMARIONessuna valutazione finora
- COVID19 HandookDocumento86 pagineCOVID19 HandookRagavNessuna valutazione finora
- Project Proposal For Don GaloDocumento20 pagineProject Proposal For Don GaloEarlNessuna valutazione finora
- Position PaperDocumento5 paginePosition PaperPrecious IgnacioNessuna valutazione finora
- 24-06-2020 HMB EnglishDocumento20 pagine24-06-2020 HMB EnglishRakshith GowdaNessuna valutazione finora
- RBI-Week 5 Q2Documento9 pagineRBI-Week 5 Q2Jay Marasigan HernandezNessuna valutazione finora
- Down and Down and Out: InsideDocumento24 pagineDown and Down and Out: InsideMohd Ilham AdamNessuna valutazione finora
- IPO Note - Krsnaa Diagnostics LimitedDocumento16 pagineIPO Note - Krsnaa Diagnostics LimitedRajan Babu SNessuna valutazione finora
- Covid CertificateDocumento3 pagineCovid CertificateanmolNessuna valutazione finora
- Red Cross Blood DrivesDocumento12 pagineRed Cross Blood DrivesWJZNessuna valutazione finora
- Do2020-0406 RevisedSPMS July2020Documento69 pagineDo2020-0406 RevisedSPMS July2020Harby Ongbay AbellanosaNessuna valutazione finora
- Reopening Church After CovidDocumento26 pagineReopening Church After CovidhmareidNessuna valutazione finora
- Eng 7 Q2 Module 2 REVISEDDocumento10 pagineEng 7 Q2 Module 2 REVISEDMaria Fe Vibar100% (1)
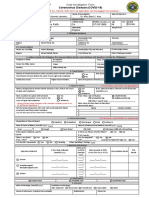
- DOH PIDSR COVID-19 CIF TemplateDocumento1 paginaDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNessuna valutazione finora
- Disaster Readiness and Risk Reduction: Disasters and Its Effects Learning From Weakness Why Us? Not Others?Documento8 pagineDisaster Readiness and Risk Reduction: Disasters and Its Effects Learning From Weakness Why Us? Not Others?Eli67% (12)
- Health Declaration Form Health Declaration Form: Respondent Information Respondent InformationDocumento2 pagineHealth Declaration Form Health Declaration Form: Respondent Information Respondent InformationErnilyn Espinosa LiganNessuna valutazione finora
- German Panic Paper 4 - Necessary Measures For Germany To Contain The COVID-19 Pandemic and To Avoid Social Collateral Damage (English)Documento9 pagineGerman Panic Paper 4 - Necessary Measures For Germany To Contain The COVID-19 Pandemic and To Avoid Social Collateral Damage (English)MichaelNessuna valutazione finora
- Coronavirus - Six Months After Pandemic Declared, Where Are The Global Hotspots - BBC NewsDocumento18 pagineCoronavirus - Six Months After Pandemic Declared, Where Are The Global Hotspots - BBC Newslockleong93Nessuna valutazione finora
- Health Assessment - Activity 1 PDFDocumento5 pagineHealth Assessment - Activity 1 PDFknotstmNessuna valutazione finora
- 007 GB A Argene Covid19 RespiratoryDocumento2 pagine007 GB A Argene Covid19 RespiratorySachinNessuna valutazione finora
- Guidance For Fully Vaccinated PeopleDocumento6 pagineGuidance For Fully Vaccinated PeopleJim Hoft0% (1)
- REV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKIDocumento22 pagineREV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKILilik AndayatiNessuna valutazione finora
- Covid-19 and BusinessDocumento4 pagineCovid-19 and BusinessAbid FerdowsNessuna valutazione finora
- Blood Clotting Disorder Reports Following Covid VaccineDocumento70 pagineBlood Clotting Disorder Reports Following Covid VaccineJosh SingerNessuna valutazione finora
- Factsheet Covid 19 Environmental CleaningDocumento2 pagineFactsheet Covid 19 Environmental CleaningsNessuna valutazione finora
- Telemedicine Conference 15 Des 2020Documento4 pagineTelemedicine Conference 15 Des 2020rafaelNessuna valutazione finora