Potrebbero piacerti anche
- Iosh Chiltern A Guide To Respiratory Protection Devices PDF EngpDocumento40 pagineIosh Chiltern A Guide To Respiratory Protection Devices PDF EngpMuhammadNessuna valutazione finora
- Despite Precautions Taken by Dental Office Staff To Keep The Office Clean and To Practice Environmental AsepsisDocumento9 pagineDespite Precautions Taken by Dental Office Staff To Keep The Office Clean and To Practice Environmental AsepsisSatnam BajwaNessuna valutazione finora
- Vacuum Aerosol 7Documento11 pagineVacuum Aerosol 7khamilatusyNessuna valutazione finora
- Iosh Respiratory Protection Webinar Presentation 2018Documento52 pagineIosh Respiratory Protection Webinar Presentation 2018MuhammadNessuna valutazione finora
- New Advances in Caries RemovalDocumento45 pagineNew Advances in Caries Removalyogi_2311Nessuna valutazione finora
- Journal of Dentistry: SciencedirectDocumento9 pagineJournal of Dentistry: SciencedirectkittyNessuna valutazione finora
- HVAC Management For Covid 19 Trans1Documento78 pagineHVAC Management For Covid 19 Trans1Santi YuliandariNessuna valutazione finora
- Scandmist Main Brochure enDocumento16 pagineScandmist Main Brochure enfluos2012Nessuna valutazione finora
- Aerosoles GlosarioDocumento2 pagineAerosoles GlosarioBJ CarminatorNessuna valutazione finora
- Puresaneo® Air Purifier - SterilizerDocumento11 paginePuresaneo® Air Purifier - SterilizerDan ZoltnerNessuna valutazione finora
- Explanation On MasksDocumento5 pagineExplanation On Masksabdulsamir3Nessuna valutazione finora
- ENDO ReportDocumento3 pagineENDO ReportReden Calubayan OblenaNessuna valutazione finora
- AB59 Tri Dim Corona Virus Control v4Documento2 pagineAB59 Tri Dim Corona Virus Control v4Luis MirandaNessuna valutazione finora
- The Role of Active Air Disinfection in Mitigating The Effects of Aerosol Generating Dental ProceduresDocumento26 pagineThe Role of Active Air Disinfection in Mitigating The Effects of Aerosol Generating Dental ProceduresAleksandraNessuna valutazione finora
- La Aparición de Esporas de Moho en El Aire Puede Prevenirse en-USDocumento2 pagineLa Aparición de Esporas de Moho en El Aire Puede Prevenirse en-USSamuel CalzadillaNessuna valutazione finora
- Macam Isolasi TambahanDocumento2 pagineMacam Isolasi TambahanDella SufyNessuna valutazione finora
- Respiratory Protection For Airborne Exposures To Biohazards: Release 3, February 2020 #174Documento9 pagineRespiratory Protection For Airborne Exposures To Biohazards: Release 3, February 2020 #174gaboinklNessuna valutazione finora
- Office of PSA - StopTheTransmission - CrushThePandemicDocumento13 pagineOffice of PSA - StopTheTransmission - CrushThePandemicDebNessuna valutazione finora
- HVAC Management For Covid 19 Trans1Documento85 pagineHVAC Management For Covid 19 Trans1FioriAmeliaHathawayNessuna valutazione finora
- Study - Scientifically Innovative Solution To Reducing Coronavirus Transmission (Shahid-Nasir July 2020)Documento14 pagineStudy - Scientifically Innovative Solution To Reducing Coronavirus Transmission (Shahid-Nasir July 2020)Fatima ShahidNessuna valutazione finora
- Association of American Physicians and SurgeonsDocumento6 pagineAssociation of American Physicians and SurgeonsDavidNessuna valutazione finora
- Respirators and Dust HazardsDocumento30 pagineRespirators and Dust HazardsKay AayNessuna valutazione finora
- Metered Dose Inhalers and Spacer Devices: C. TerzanoDocumento11 pagineMetered Dose Inhalers and Spacer Devices: C. TerzanoDwi MindriNessuna valutazione finora
- A Versatile Mistblower Attachment For Low and Ultra Low Volume SprayingDocumento2 pagineA Versatile Mistblower Attachment For Low and Ultra Low Volume SprayingMaria MorenoNessuna valutazione finora
- Fluid Control and Soft Tissue ManagementDocumento52 pagineFluid Control and Soft Tissue ManagementDeepthi Rajesh50% (2)
- 潔淨協會研討會議程2020Documento5 pagine潔淨協會研討會議程2020Yen YenNessuna valutazione finora
- Respirator Types: N95 Vs FFP3 Vs FFP2 Masks - What's The Difference? Masks Vs RespiratorsDocumento31 pagineRespirator Types: N95 Vs FFP3 Vs FFP2 Masks - What's The Difference? Masks Vs RespiratorsMaryantiNessuna valutazione finora
- Cochran 1989 - Isolamento Absoluto e Controle Da ContaminaçãoDocumento4 pagineCochran 1989 - Isolamento Absoluto e Controle Da ContaminaçãoGifix GifunNessuna valutazione finora
- Kartika Indira PutriDocumento7 pagineKartika Indira PutriKartika IndiraNessuna valutazione finora
- Dust and Its ControlDocumento6 pagineDust and Its ControlLeighton KendelyNessuna valutazione finora
- Vacuum Aerosol 2Documento14 pagineVacuum Aerosol 2khamilatusyNessuna valutazione finora
- Gumarny Zubri OM 90 Mask SpecificationDocumento3 pagineGumarny Zubri OM 90 Mask SpecificationCaramiafanNessuna valutazione finora
- Medical Face Mask and Diagnostic Kit For CoronavirusDocumento28 pagineMedical Face Mask and Diagnostic Kit For CoronavirusAngel YapNessuna valutazione finora
- Respiratory Protection For Airborne Exposures To Biohazards - TDB174Documento10 pagineRespiratory Protection For Airborne Exposures To Biohazards - TDB174indianalagNessuna valutazione finora
- SANITIZING TUNNEL PPT FinalDocumento12 pagineSANITIZING TUNNEL PPT FinalSOUMYA HNessuna valutazione finora
- Review Article Aerosol Suction Device: Mandatory Armamentarium in Dentistry Post Lock DownDocumento4 pagineReview Article Aerosol Suction Device: Mandatory Armamentarium in Dentistry Post Lock DownAlya DayNessuna valutazione finora
- Mask Information SheetDocumento4 pagineMask Information SheetPipsNessuna valutazione finora
- Surface Disinfection: Choosing The Right DisinfectantDocumento3 pagineSurface Disinfection: Choosing The Right DisinfectantSanti utamiNessuna valutazione finora
- Removal Techniques For Intracanal Medicament-A ReviewDocumento5 pagineRemoval Techniques For Intracanal Medicament-A ReviewMohammad YousifNessuna valutazione finora
- The Validation of The Sterinis Machine: at Adelaide Meath Hospital, Tallaght, DublinDocumento21 pagineThe Validation of The Sterinis Machine: at Adelaide Meath Hospital, Tallaght, DublinLowayNessuna valutazione finora
- For Pre-Final DefenseDocumento12 pagineFor Pre-Final DefenseYlizia AuburnNessuna valutazione finora
- Your Trusted Solution For A Sterile EnvironmentDocumento10 pagineYour Trusted Solution For A Sterile EnvironmentSanjay SharmaNessuna valutazione finora
- Effects of Preprocedural Mouth Rinse On Microbial.12Documento7 pagineEffects of Preprocedural Mouth Rinse On Microbial.12samanvi badriNessuna valutazione finora
- Drill Less Air AbrasionDocumento4 pagineDrill Less Air AbrasionMaria IvanaNessuna valutazione finora
- Dinio Rad ProtectionDocumento5 pagineDinio Rad ProtectionLalaine De JesusNessuna valutazione finora
- Che3261 Duran Midterm-AssignmentDocumento5 pagineChe3261 Duran Midterm-AssignmentCyberR.DomingoNessuna valutazione finora
- MSDS of N 9901Documento12 pagineMSDS of N 9901Seno BuminusaNessuna valutazione finora
- ALEz-01-COSHH Assessment Thioflz ALEz-01Documento2 pagineALEz-01-COSHH Assessment Thioflz ALEz-01Siyadarakkalmajeed ArakkalmajeedNessuna valutazione finora
- Dr. Hygiene Company ProfileDocumento12 pagineDr. Hygiene Company ProfileShubhodeep DasNessuna valutazione finora
- Ext-Cm-1081 FT - Surfa Safe SHDocumento2 pagineExt-Cm-1081 FT - Surfa Safe SHJessika VargasNessuna valutazione finora
- Disrupting The Transmission of Influenza A Face Ma PDFDocumento7 pagineDisrupting The Transmission of Influenza A Face Ma PDFBen SenNessuna valutazione finora
- Disrupting The Transmission of Influenza A Face Ma PDFDocumento7 pagineDisrupting The Transmission of Influenza A Face Ma PDFBen SenNessuna valutazione finora
- Che3261 - Domingo, Duran, Fernandez - Midterm-AssignmentDocumento5 pagineChe3261 - Domingo, Duran, Fernandez - Midterm-AssignmentCyberR.DomingoNessuna valutazione finora
- Livinguard Respirators - Coronavirus 20200219Documento10 pagineLivinguard Respirators - Coronavirus 20200219MutiaraDaraNessuna valutazione finora
- Surgical N95 vs. Standard N95 - Which To Consider?: DescriptionDocumento3 pagineSurgical N95 vs. Standard N95 - Which To Consider?: DescriptionpremNessuna valutazione finora
- Aerosol A Silent Killer in Dental PracticeDocumento5 pagineAerosol A Silent Killer in Dental PracticedehaaNessuna valutazione finora
- Vacuum Aerosol 6Documento7 pagineVacuum Aerosol 6khamilatusyNessuna valutazione finora
- Oral and Maxillofacial Surgery in Covid-19 Era A Review ArticleDocumento5 pagineOral and Maxillofacial Surgery in Covid-19 Era A Review ArticleInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Aseptix Aerox TPSDocumento4 pagineAseptix Aerox TPSUtkarsh RaiNessuna valutazione finora
- Principles and Practices of Contamination Control and CleanroomsDa EverandPrinciples and Practices of Contamination Control and CleanroomsNessuna valutazione finora
- 2022 State of Medical Device ReportDocumento38 pagine2022 State of Medical Device ReportDiego A Echavarría ANessuna valutazione finora
- Quality Assessment of The University Classroom Lighting - A Case StudyDocumento8 pagineQuality Assessment of The University Classroom Lighting - A Case StudyDiego A Echavarría ANessuna valutazione finora
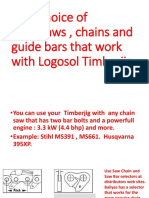
- Your Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDocumento6 pagineYour Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDiego A Echavarría ANessuna valutazione finora
- MHAC-An Assessment Tool For Analysing Manual Material Handling TasksDocumento14 pagineMHAC-An Assessment Tool For Analysing Manual Material Handling TasksDiego A Echavarría ANessuna valutazione finora
- Task AnalisisDocumento43 pagineTask AnalisisDiego A Echavarría ANessuna valutazione finora
- A Literature Review of The Effects of Natural Light On Building OccupantsDocumento58 pagineA Literature Review of The Effects of Natural Light On Building OccupantsDiego A Echavarría ANessuna valutazione finora
- Assessment of The Ergonomic Risk From Saddle and CDocumento14 pagineAssessment of The Ergonomic Risk From Saddle and CDiego A Echavarría ANessuna valutazione finora
- Overview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDocumento1 paginaOverview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDiego A Echavarría ANessuna valutazione finora
- Workplace Ergonomic Guide Darcor Final January 2015Documento14 pagineWorkplace Ergonomic Guide Darcor Final January 2015Diego A Echavarría ANessuna valutazione finora
- Validity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Documento10 pagineValidity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Diego A Echavarría ANessuna valutazione finora
- Daylight and The Workplace Study: Your Window To WellnessDocumento12 pagineDaylight and The Workplace Study: Your Window To WellnessDiego A Echavarría ANessuna valutazione finora
- Human Centric Lighting: Ir. Jasmien Vander Beken January 2019Documento13 pagineHuman Centric Lighting: Ir. Jasmien Vander Beken January 2019Diego A Echavarría ANessuna valutazione finora
- Visual Ergonomics in The Workplace: Vision and LightingDocumento11 pagineVisual Ergonomics in The Workplace: Vision and LightingDiego A Echavarría ANessuna valutazione finora
- Design Principles For Green Ergonomics: April 2013Documento6 pagineDesign Principles For Green Ergonomics: April 2013Diego A Echavarría ANessuna valutazione finora
- Visual Ergonomics: Solutions For Lighting & Eye Health: Tel: 604-822-9040 Fax: 604-822-0572 Ergonomics - Info@ubc - CaDocumento7 pagineVisual Ergonomics: Solutions For Lighting & Eye Health: Tel: 604-822-9040 Fax: 604-822-0572 Ergonomics - Info@ubc - CaDiego A Echavarría ANessuna valutazione finora
- The Effects of Exposure To Natural Light in The.5Documento19 pagineThe Effects of Exposure To Natural Light in The.5Diego A Echavarría ANessuna valutazione finora
- The Benefits of Natural Light: January-February 2014Documento3 pagineThe Benefits of Natural Light: January-February 2014Diego A Echavarría ANessuna valutazione finora
- Daylight For Health and Efficiency - A New Career For An Old FriendDocumento8 pagineDaylight For Health and Efficiency - A New Career For An Old FriendDiego A Echavarría ANessuna valutazione finora
- Hung Et Al-2009-Human Factors and Ergonomics in Manufacturing & Service Industries PDFDocumento16 pagineHung Et Al-2009-Human Factors and Ergonomics in Manufacturing & Service Industries PDFDiego A Echavarría ANessuna valutazione finora
- b531 PDFDocumento14 pagineb531 PDFDiego A Echavarría ANessuna valutazione finora
- Visual Ergonomics in The Workplace: Continuing EducationDocumento7 pagineVisual Ergonomics in The Workplace: Continuing EducationDiego A Echavarría ANessuna valutazione finora
- Task Lighting Solutions: Their Economic and Ergonomic BenefitsDocumento8 pagineTask Lighting Solutions: Their Economic and Ergonomic BenefitsDiego A Echavarría ANessuna valutazione finora
- Dhs - Oha: Office Light Management GuideDocumento17 pagineDhs - Oha: Office Light Management GuideDiego A Echavarría ANessuna valutazione finora
- Optometry: From Visual Performance To Visual Ergonomics: A Personal Historic ViewDocumento7 pagineOptometry: From Visual Performance To Visual Ergonomics: A Personal Historic ViewDiego A Echavarría ANessuna valutazione finora
- Can The Office Environment Stimulate A Manager's Creativity?Documento14 pagineCan The Office Environment Stimulate A Manager's Creativity?Diego A Echavarría ANessuna valutazione finora
- SSL Trajectories Proc IEEEDocumento18 pagineSSL Trajectories Proc IEEEDiego A Echavarría ANessuna valutazione finora
- E3sconf hrc2018 02017Documento5 pagineE3sconf hrc2018 02017Diego A Echavarría ANessuna valutazione finora
- Synergies Between Ergoecology and Green Ergonomics: A Contribution Towards A Sustainability Agenda For HFEDocumento6 pagineSynergies Between Ergoecology and Green Ergonomics: A Contribution Towards A Sustainability Agenda For HFEDiego A Echavarría ANessuna valutazione finora
- Visual Ergonomics at Work and Leisure: Paying It ForwardDocumento2 pagineVisual Ergonomics at Work and Leisure: Paying It ForwardDiego A Echavarría ANessuna valutazione finora
- Lighting Design in Workplaces: A Case Study of A Modern Library Building in Sheffield, UKDocumento8 pagineLighting Design in Workplaces: A Case Study of A Modern Library Building in Sheffield, UKDiego A Echavarría ANessuna valutazione finora
- Circular Economy, The Concept and It's LimitationsDocumento10 pagineCircular Economy, The Concept and It's LimitationsCésar De La Cruz OlivaNessuna valutazione finora
- Final Thesis For Blocking Social Media SitesDocumento15 pagineFinal Thesis For Blocking Social Media SitesRhoebieNessuna valutazione finora
- Usiness Aluation: DigestDocumento28 pagineUsiness Aluation: Digestgioro_miNessuna valutazione finora
- One2One Panama 2015Documento6 pagineOne2One Panama 2015Dhaval ShahNessuna valutazione finora
- Tutorial #4 KL4120 Offshore Platform Ocean Engineering ITB 2015Documento26 pagineTutorial #4 KL4120 Offshore Platform Ocean Engineering ITB 2015Ockto Perdana SinagaNessuna valutazione finora
- Nano ProgrammingDocumento3 pagineNano ProgrammingBhavani DhanasekaranNessuna valutazione finora
- Research On The Jackson Personality Inventory Revised JPI R PDFDocumento16 pagineResearch On The Jackson Personality Inventory Revised JPI R PDFAndrea RosalNessuna valutazione finora
- UNIT1 Question Bank EDDocumento7 pagineUNIT1 Question Bank EDsuganya1190Nessuna valutazione finora
- MetricsDocumento50 pagineMetricsArjun VaranasiNessuna valutazione finora
- Python in A Nutshell: Python's Whys & HowsDocumento4 paginePython in A Nutshell: Python's Whys & Howstvboxsmart newNessuna valutazione finora
- Possible Test1Documento32 paginePossible Test1Azim Jivani100% (3)
- Fall Prevention and Protection ProcedureDocumento23 pagineFall Prevention and Protection Procedureibrahim100% (1)
- Report HRTP Sanofi PakistanDocumento13 pagineReport HRTP Sanofi PakistanANUS AHMED KHANNessuna valutazione finora
- Masurare Grosime Vopsea 1 - Fisa-tehnica-Extech-CG204Documento1 paginaMasurare Grosime Vopsea 1 - Fisa-tehnica-Extech-CG204RizzoRo1Nessuna valutazione finora
- Project Protocol For Organic TeaDocumento5 pagineProject Protocol For Organic TeaMuntaha ZyanNessuna valutazione finora
- FIN350 Quiz 2 Monday First Name - Last Name - Version BDocumento6 pagineFIN350 Quiz 2 Monday First Name - Last Name - Version BHella Mae RambunayNessuna valutazione finora
- Puyat V de GuzmanDocumento6 paginePuyat V de GuzmanDwight LoNessuna valutazione finora
- IOT Door Buzzer & Home Security DeviceDocumento5 pagineIOT Door Buzzer & Home Security Devicekutty vickyNessuna valutazione finora
- Wafer Check Valves - O&MDocumento4 pagineWafer Check Valves - O&MjayakumarNessuna valutazione finora
- Slab Design TWO WAY at 10.2 M TOCDocumento1 paginaSlab Design TWO WAY at 10.2 M TOCVikalp MadhavNessuna valutazione finora
- John Paulding MuseumDocumento4 pagineJohn Paulding Museumapi-316020003Nessuna valutazione finora
- HNS Level 4 Basic COC QueationDocumento17 pagineHNS Level 4 Basic COC QueationMohammed Jemal90% (10)
- T-79 4202 Solutions 4Documento4 pagineT-79 4202 Solutions 4bobopowerNessuna valutazione finora
- Huawei CX311 Switch Module V100R001C00 White Paper 09Documento41 pagineHuawei CX311 Switch Module V100R001C00 White Paper 09zain_zedanNessuna valutazione finora
- Saved-20220203 1028 25955Documento14 pagineSaved-20220203 1028 25955Akshay GautamNessuna valutazione finora
- Energies 10 02018 PDFDocumento20 pagineEnergies 10 02018 PDFيوليسيس أوريروNessuna valutazione finora
- FaDocumento20 pagineFaVishwanath ShervegarNessuna valutazione finora
- Four Daewoo Motors Ex-Executives Acquitted of Fraud Charges - The Economic TimesDocumento1 paginaFour Daewoo Motors Ex-Executives Acquitted of Fraud Charges - The Economic TimescreateNessuna valutazione finora
- Følstad & Brandtzaeg (2020)Documento14 pagineFølstad & Brandtzaeg (2020)Ijlal Shidqi Al KindiNessuna valutazione finora
- Jcss Probabilistic Modelcode Part 3: Resistance ModelsDocumento4 pagineJcss Probabilistic Modelcode Part 3: Resistance Modelsdimitrios25Nessuna valutazione finora