Potrebbero piacerti anche
- State of The Art Concepts in Aortic Valve Replacement: Please Join Us For The 90 MinutesDocumento1 paginaState of The Art Concepts in Aortic Valve Replacement: Please Join Us For The 90 MinutesEthan AmalNessuna valutazione finora
- Parental Care and The Development of The Parent Offspring Conflict in Discus Fish (Symphysodon SPP.)Documento298 pagineParental Care and The Development of The Parent Offspring Conflict in Discus Fish (Symphysodon SPP.)Ethan AmalNessuna valutazione finora
- Edwards iBAR Agenda 16thoct ThailandDocumento1 paginaEdwards iBAR Agenda 16thoct ThailandEthan AmalNessuna valutazione finora
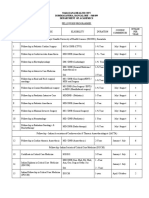
- Narayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsDocumento2 pagineNarayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsEthan AmalNessuna valutazione finora
- Page Proof Instructions and Queries: Asian Cardiovascular & Thoracic Annals (AAN) 984097Documento6 paginePage Proof Instructions and Queries: Asian Cardiovascular & Thoracic Annals (AAN) 984097Ethan AmalNessuna valutazione finora
- AA Issue-Article 9Documento11 pagineAA Issue-Article 9Ethan AmalNessuna valutazione finora
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocumento35 pagineWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEthan AmalNessuna valutazione finora
- Ccam N Bps Management PDFDocumento9 pagineCcam N Bps Management PDFEthan AmalNessuna valutazione finora
- Safety of Temporary Pacemaker WiresDocumento20 pagineSafety of Temporary Pacemaker WiresEthan AmalNessuna valutazione finora
- Av Shunt Mabi XXDocumento33 pagineAv Shunt Mabi XXEthan AmalNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Interest GroupsDocumento25 pagineInterest GroupsnikkivNessuna valutazione finora
- Visual Interpretation QuestionsDocumento7 pagineVisual Interpretation Questionssoomro76134Nessuna valutazione finora
- Maraging Steels - Making Steel Strong and CheapDocumento3 pagineMaraging Steels - Making Steel Strong and CheapSlamet Tribudi PrakosoNessuna valutazione finora
- Catholic Vicar Vs CA, 555Documento11 pagineCatholic Vicar Vs CA, 555Lee SomarNessuna valutazione finora
- 09Documento69 pagine09Sakshi VermaNessuna valutazione finora
- Backgrounder 4 (Ahmad & Tank 2021) - Sharia Law and Women's RightsDocumento6 pagineBackgrounder 4 (Ahmad & Tank 2021) - Sharia Law and Women's RightsaminNessuna valutazione finora
- Enoch 2 PDFDocumento164 pagineEnoch 2 PDFJesse Glaser50% (4)
- CHEM BIO Organic MoleculesDocumento7 pagineCHEM BIO Organic MoleculesLawrence SarmientoNessuna valutazione finora
- Chams 1Documento78 pagineChams 1Das RavindraNessuna valutazione finora
- Unit: 2 States of Matter: Important PointsDocumento24 pagineUnit: 2 States of Matter: Important PointsManish SinghNessuna valutazione finora
- AIP Chapter FiveDocumento113 pagineAIP Chapter Fivetekalegn barekuNessuna valutazione finora
- The Urantia Book (Public Domain)Documento1.806 pagineThe Urantia Book (Public Domain)Lenny100% (13)
- 4 - Bit Shift RegisterDocumento32 pagine4 - Bit Shift RegisterPooja PantNessuna valutazione finora
- Marketing Management A Strategic Decision Making Approach 8th Edition Mullins Test BankDocumento36 pagineMarketing Management A Strategic Decision Making Approach 8th Edition Mullins Test Bankivanjordang11k7i100% (26)
- Negotiation and Diplomacy Term PaperDocumento37 pagineNegotiation and Diplomacy Term PaperManifa OsmanNessuna valutazione finora
- Thermo. عبدالله رعد حران - 32Documento4 pagineThermo. عبدالله رعد حران - 32عبدالله رعد حران 32Nessuna valutazione finora
- 15 UtilitarianismDocumento25 pagine15 UtilitarianismGracelyn CablayNessuna valutazione finora
- Assignment Topic: Under The Supervision of Mam SehrishDocumento18 pagineAssignment Topic: Under The Supervision of Mam SehrishAttarehman QureshiNessuna valutazione finora
- Literature of Cagayan ValleyDocumento30 pagineLiterature of Cagayan ValleyCara DonafrioNessuna valutazione finora
- Competing Values Quinn and Cameron (1) ++++Documento182 pagineCompeting Values Quinn and Cameron (1) ++++fishermanalu100% (1)
- Growth of The SocialismDocumento11 pagineGrowth of The SocialismHarpreet SinghNessuna valutazione finora
- Activity 1: Making A Simple Rapid Curriculum EvaluationDocumento9 pagineActivity 1: Making A Simple Rapid Curriculum EvaluationShainnah Cawa75% (4)
- English Prototype Paper Ordinary LevelDocumento13 pagineEnglish Prototype Paper Ordinary LevelBruce Wayne83% (6)
- Academic Calendar Winter VIT 2020-21Documento1 paginaAcademic Calendar Winter VIT 2020-21ShubhamNessuna valutazione finora
- Section Intergroup Conflict TheoriesDocumento5 pagineSection Intergroup Conflict Theoriesar009baNessuna valutazione finora
- E Commerce SecurityDocumento5 pagineE Commerce SecurityAhmed KhalafNessuna valutazione finora
- Cawis vs. Cerilles - G.R. No. 170207 - April 19, 2010Documento2 pagineCawis vs. Cerilles - G.R. No. 170207 - April 19, 2010Lordy Jessah AggabaoNessuna valutazione finora
- Fakultas Kedokteran Universitas Islam Sultan Agung SemarangDocumento17 pagineFakultas Kedokteran Universitas Islam Sultan Agung SemarangTyar Bhatara PutraNessuna valutazione finora
- Ele Imhpssdp 1ST Term NotesDocumento7 pagineEle Imhpssdp 1ST Term NotesDANIELLE TORRANCE ESPIRITUNessuna valutazione finora
- Is The Legend of Oedipus A FolktaleDocumento12 pagineIs The Legend of Oedipus A FolktaleLuciano CabralNessuna valutazione finora