Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Master Youtube: WorkbookDocumento64 pagineMaster Youtube: WorkbookLucian TrandafirNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Review of Related LiteratureDocumento27 pagineReview of Related Literatureme langNessuna valutazione finora
- Site Planning: by TonjaDocumento60 pagineSite Planning: by Tonjabisrat meseretNessuna valutazione finora
- Chapter 1-2Documento25 pagineChapter 1-2bisrat meseretNessuna valutazione finora
- Introduction To Economics: By: Tewolde GDocumento50 pagineIntroduction To Economics: By: Tewolde Gbisrat meseretNessuna valutazione finora
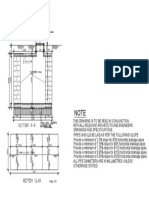
- Detail Sectttt PDFDocumento1 paginaDetail Sectttt PDFbisrat meseretNessuna valutazione finora
- Man Hole DetaaDocumento1 paginaMan Hole Detaabisrat meseretNessuna valutazione finora
- Introduction To Economics (ECON.101) : By: Fasil EDocumento20 pagineIntroduction To Economics (ECON.101) : By: Fasil Ebisrat meseretNessuna valutazione finora
- Types of Wood Lec-1Documento5 pagineTypes of Wood Lec-1bisrat meseretNessuna valutazione finora
- Lecture 4Documento44 pagineLecture 4bisrat meseretNessuna valutazione finora
- Site Analysis FrameworkDocumento9 pagineSite Analysis Frameworkbisrat meseretNessuna valutazione finora
- Principles of Curtain WallingDocumento16 paginePrinciples of Curtain Wallingjewon100% (1)
- Introduction To Environmental Planning: Lecture TwoDocumento37 pagineIntroduction To Environmental Planning: Lecture Twobisrat meseretNessuna valutazione finora
- Town Planning ReportDocumento27 pagineTown Planning Reportمنير أحمدNessuna valutazione finora
- Introduction To Environmental PlanningDocumento31 pagineIntroduction To Environmental Planningbisrat meseretNessuna valutazione finora
- Installation Manual - CurtainWall OpeningsDocumento10 pagineInstallation Manual - CurtainWall OpeningsManh NguyenNessuna valutazione finora
- SAS Curtain Wall BrochureDocumento28 pagineSAS Curtain Wall BrochureAngga RamadhanNessuna valutazione finora
- Lecture 7 & 8 Ordering PrinciplesDocumento19 pagineLecture 7 & 8 Ordering Principlesbisrat meseretNessuna valutazione finora
- Lecture 7 & 8 Ordering PrinciplesDocumento19 pagineLecture 7 & 8 Ordering Principlesbisrat meseretNessuna valutazione finora
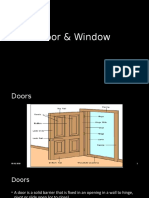
- Door & WindowDocumento16 pagineDoor & Windowbisrat meseretNessuna valutazione finora
- Door & WindowDocumento16 pagineDoor & Windowbisrat meseretNessuna valutazione finora
- Chimneys and Fireplaces: 2003 International Residential Codex 263Documento10 pagineChimneys and Fireplaces: 2003 International Residential Codex 263bisrat meseretNessuna valutazione finora
- Curtain Wall Installation Instructions - Rev 05-04-11Documento36 pagineCurtain Wall Installation Instructions - Rev 05-04-11rmdarisaNessuna valutazione finora
- A Curtain Wall System Is An Outer Covering of A Building in Which The Outer Walls Are NonDocumento23 pagineA Curtain Wall System Is An Outer Covering of A Building in Which The Outer Walls Are Nonbisrat meseretNessuna valutazione finora
- A Curtain Wall System Is An Outer Covering of A Building in Which The Outer Walls Are NonDocumento23 pagineA Curtain Wall System Is An Outer Covering of A Building in Which The Outer Walls Are Nonbisrat meseretNessuna valutazione finora
- Building Material Connection Details DrawingsDocumento10 pagineBuilding Material Connection Details Drawingsbisrat meseretNessuna valutazione finora
- Curtain Wall Installation HandbookDocumento34 pagineCurtain Wall Installation HandbookAbdul RaqeebNessuna valutazione finora
- Building Spatial Design Final SecuredDocumento70 pagineBuilding Spatial Design Final Securedephrem100% (1)
- Building Spatial Design Final SecuredDocumento70 pagineBuilding Spatial Design Final Securedephrem100% (1)
- 1.1 Background of The Study: Chapter OneDocumento34 pagine1.1 Background of The Study: Chapter Onebisrat meseret0% (1)
- 2020 Ethiopian Standards Catalogue PDFDocumento25 pagine2020 Ethiopian Standards Catalogue PDFbisrat meseret50% (6)
- Integration of Traditional and Modern Market SpaceDocumento37 pagineIntegration of Traditional and Modern Market Spacebisrat meseretNessuna valutazione finora
- Test Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithDocumento17 pagineTest Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W Smithwoodwardpunction2vq46zNessuna valutazione finora
- Disorders of The Nervous System2Documento20 pagineDisorders of The Nervous System2Ian Rizavi Villamor AntopinaNessuna valutazione finora
- Phys113 Notes 9Documento4 paginePhys113 Notes 9Manuel DiazNessuna valutazione finora
- Social Content GuidelinesDocumento24 pagineSocial Content GuidelinesPrincess Kylah Chua TorresNessuna valutazione finora
- West Philippine SeaDocumento4 pagineWest Philippine SeaFrancheskalane ValenciaNessuna valutazione finora
- Task Risk Assessment FormDocumento1 paginaTask Risk Assessment Formmuhammadsuhaib100% (1)
- Update CV Hse Engineer SlimaniDocumento3 pagineUpdate CV Hse Engineer SlimanialiouecheNessuna valutazione finora
- Five Times Sit To Stand (5Tsts) : InstructionsDocumento2 pagineFive Times Sit To Stand (5Tsts) : InstructionsNovinna KusumawatiNessuna valutazione finora
- Challenging The Stigma of Mental Illness Among College StudentsDocumento7 pagineChallenging The Stigma of Mental Illness Among College StudentsJene ArcegaNessuna valutazione finora
- HSE Final Group 9Documento9 pagineHSE Final Group 9Rohan NandiNessuna valutazione finora
- 4 Ethical Choices in BusinessDocumento34 pagine4 Ethical Choices in BusinessE-ሽገር Online bussinessNessuna valutazione finora
- Publicação 2Documento8 paginePublicação 2BrunoNessuna valutazione finora
- Evaluation of Scientific Publications - Part 22 - Estimation of Effects in The Absence of Head-to-Head Trials PDFDocumento6 pagineEvaluation of Scientific Publications - Part 22 - Estimation of Effects in The Absence of Head-to-Head Trials PDFPhoNessuna valutazione finora
- Hijama Cupping PDFDocumento16 pagineHijama Cupping PDFMuhammad Khalid JavedNessuna valutazione finora
- Sales Leads - StillorganDocumento10 pagineSales Leads - StillorganDarko PanevNessuna valutazione finora
- Final Record SCT - 2037558Documento14 pagineFinal Record SCT - 2037558Aiswarya VenkataramananNessuna valutazione finora
- Byram Enteral - NutritionDocumento7 pagineByram Enteral - NutritionGrace XieNessuna valutazione finora
- The Role of Health and Education and Economic Growth of PakistanDocumento68 pagineThe Role of Health and Education and Economic Growth of PakistankamilbismaNessuna valutazione finora
- I Have Nothing - Brass - TrumpetDocumento1 paginaI Have Nothing - Brass - TrumpetMiguel Rodrigo Estrada GutierrezNessuna valutazione finora
- Communicating Across CulturesDocumento2 pagineCommunicating Across CulturesDnyaneshwar PatilNessuna valutazione finora
- WSBB Guide For Beginners - Bench-CompressedDocumento15 pagineWSBB Guide For Beginners - Bench-CompressedKatya KNessuna valutazione finora
- Module 6 Performance AppraisalDocumento8 pagineModule 6 Performance AppraisalAngel Calipdan ValdezNessuna valutazione finora
- Abnormal Psychology TestDocumento19 pagineAbnormal Psychology TestJona MaeNessuna valutazione finora
- Latest Memo From Howard Marks: Which Way Now?: Archived MemosDocumento16 pagineLatest Memo From Howard Marks: Which Way Now?: Archived MemoscoolchadsNessuna valutazione finora
- Fire Risk Assessment TemplatesDocumento38 pagineFire Risk Assessment Templateskhalid najjarNessuna valutazione finora
- BC Public Service Covid19 Response FaqsDocumento22 pagineBC Public Service Covid19 Response FaqsPuRe Sp3ctreNessuna valutazione finora
- VISUAL PERCEPTION DISORDER HandoutsDocumento3 pagineVISUAL PERCEPTION DISORDER HandoutsJemuel Bucud LagartoNessuna valutazione finora
- Ways of CopingDocumento5 pagineWays of Copingteena jobNessuna valutazione finora