Potrebbero piacerti anche
- Endodontic MCQ PDFDocumento17 pagineEndodontic MCQ PDFYousef Hussain Ghannam89% (66)
- A26 - Walk in Paschim Vihar Ii: NoteDocumento2 pagineA26 - Walk in Paschim Vihar Ii: NoteLakshay MahajanNessuna valutazione finora
- Anemia Pada Anak - DR AuliaDocumento61 pagineAnemia Pada Anak - DR AuliaSamuel ManurungNessuna valutazione finora
- Hematologi ModulDocumento67 pagineHematologi ModulSyifa Mahmud Syukran Akbar100% (1)
- Outline: Anaemias I Microcytic, Iron Deficiency Microcytic, Iron Deficiency & Iron OverloadDocumento11 pagineOutline: Anaemias I Microcytic, Iron Deficiency Microcytic, Iron Deficiency & Iron Overloaddorsa koraeiNessuna valutazione finora
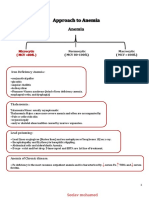
- Approach To AnemiaDocumento4 pagineApproach To AnemiapNessuna valutazione finora
- AnaemiaDocumento25 pagineAnaemiaIshali NuwanjiniNessuna valutazione finora
- Anemia DM-1 - REV.Documento44 pagineAnemia DM-1 - REV.abdulrahmanbelewa96Nessuna valutazione finora
- Hematology SBIM Part 1Documento7 pagineHematology SBIM Part 1Gousay AlkhazmariNessuna valutazione finora
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocumento500 pagineSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNessuna valutazione finora
- BoardReviewPart1A BenignHemePathDocumento170 pagineBoardReviewPart1A BenignHemePathMaria Cristina Alarcon NietoNessuna valutazione finora
- Finals Week 10Documento8 pagineFinals Week 10MARIE NELLIE MOSTRADONessuna valutazione finora
- Anemia Dalam Kehamilan-OliviaDocumento20 pagineAnemia Dalam Kehamilan-OliviaSwitha Martha Sinaga100% (1)
- Hemolytic Anemia, Types, and SymotomsDocumento3 pagineHemolytic Anemia, Types, and SymotomsNada AmjadNessuna valutazione finora
- Degenevie - HematologyDocumento71 pagineDegenevie - Hematologykkq7fhkwvkNessuna valutazione finora
- Patho HematologyDocumento39 paginePatho HematologyCastleKGNessuna valutazione finora
- RBC anomalies-ANEMIADocumento19 pagineRBC anomalies-ANEMIAJeremiahNessuna valutazione finora
- MSN I 12.6.2020 FN Unit V Megaloblastic Anemia & Aplastic AnemiaDocumento44 pagineMSN I 12.6.2020 FN Unit V Megaloblastic Anemia & Aplastic AnemiaHariniNessuna valutazione finora
- AnemiaDocumento7 pagineAnemiaMaria Jose BravoNessuna valutazione finora
- Pendekatan Diagnosis AnemiaDocumento7 paginePendekatan Diagnosis AnemiaFerry GhifariNessuna valutazione finora
- Nursing Clients With Hematologic DisordersDocumento4 pagineNursing Clients With Hematologic DisordersLuna MarieNessuna valutazione finora
- HematologyDocumento20 pagineHematologyJunaid SabirNessuna valutazione finora
- Hematology Trans 10Documento6 pagineHematology Trans 10Claire GonoNessuna valutazione finora
- Anemia - AmbossDocumento10 pagineAnemia - AmbossGuga XachidzeNessuna valutazione finora
- AnemiaDocumento7 pagineAnemiaoktavianprNessuna valutazione finora
- Physiology Lab V2Documento14 paginePhysiology Lab V2Mohammed EljackNessuna valutazione finora
- Anemia 2011 Student Dental FDocumento64 pagineAnemia 2011 Student Dental Fkays30002403Nessuna valutazione finora
- Anemia 2 and Malaria 1Documento30 pagineAnemia 2 and Malaria 1Aishwarya JeeNessuna valutazione finora
- Clinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDocumento24 pagineClinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDzil FikriNessuna valutazione finora
- Clasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKDocumento46 pagineClasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKrubyniNessuna valutazione finora
- AnemiaDocumento27 pagineAnemiaSri Ram Prasath TNessuna valutazione finora
- Anemia 1Documento92 pagineAnemia 1Bikash PatgiriNessuna valutazione finora
- Anemia GravisDocumento35 pagineAnemia GravisMufthifina AulahaqNessuna valutazione finora
- Rhabdomyolysis: DR - Marwa Elwasif NephrologistDocumento28 pagineRhabdomyolysis: DR - Marwa Elwasif NephrologistAbualauon AlbeblawyNessuna valutazione finora
- PediatricDocumento192 paginePediatricbolt boltNessuna valutazione finora
- Assoc of Erythrocytes With Clinical ConditionsDocumento3 pagineAssoc of Erythrocytes With Clinical ConditionsHaniGirlAlay-ayCachoNessuna valutazione finora
- Dr. Sailendra Nayak Assistant Professor MedicineDocumento49 pagineDr. Sailendra Nayak Assistant Professor MedicineAishwarya JeeNessuna valutazione finora
- Diagnosing Anemia General ConceptsDocumento111 pagineDiagnosing Anemia General ConceptsTony DawaNessuna valutazione finora
- Hematology 4Documento21 pagineHematology 4saad samyNessuna valutazione finora
- Brains Review Hematology: AnemiaDocumento173 pagineBrains Review Hematology: Anemia"DocAxi" Maximo B Axibal Jr MD FPSPNessuna valutazione finora
- AnemiaDocumento20 pagineAnemiaبشير حيدرNessuna valutazione finora
- ANEMIADocumento3 pagineANEMIAjessa tabanginNessuna valutazione finora
- Anemia of Bone Marrow FailureDocumento6 pagineAnemia of Bone Marrow FailureKim Alyssa GoNessuna valutazione finora
- AnaemiaDocumento7 pagineAnaemiaYousef El3alameyNessuna valutazione finora
- Revisi Slide Adb Lecture Koass - Dwi ADocumento23 pagineRevisi Slide Adb Lecture Koass - Dwi AGoez Aditya NugrahaNessuna valutazione finora
- Pathophysiology & Therapeutics - Anemia-Prof WoodeDocumento52 paginePathophysiology & Therapeutics - Anemia-Prof WoodeMuhammad AbdullahiNessuna valutazione finora
- Macrocytic AnemiaDocumento49 pagineMacrocytic AnemiaANessuna valutazione finora
- AnemiaDocumento55 pagineAnemiaapi-2682649650% (2)
- AnemiaDocumento96 pagineAnemiaArpita SankhwarNessuna valutazione finora
- Anemia 2024Documento50 pagineAnemia 2024b9p6vmfnc4Nessuna valutazione finora
- AnaemiaDocumento34 pagineAnaemiadakshpanchal26369Nessuna valutazione finora
- Interpreting The CBC - When To ReferDocumento44 pagineInterpreting The CBC - When To ReferKannan KannanNessuna valutazione finora
- Anemia: Prof. Dr. Djoni Djunaedi, DR., SP - PD., KptiDocumento48 pagineAnemia: Prof. Dr. Djoni Djunaedi, DR., SP - PD., KptiHarmas Novryan FarezaNessuna valutazione finora
- Pediatric Hematology & Oncology: Muhammad RizaDocumento19 paginePediatric Hematology & Oncology: Muhammad Rizaproman wazowskiNessuna valutazione finora
- Lecture 29-AnemiaDocumento35 pagineLecture 29-AnemiaBini JaminNessuna valutazione finora
- (PPT) IM (Onco and Hema)Documento78 pagine(PPT) IM (Onco and Hema)ricaannpanugalinogNessuna valutazione finora
- All HematologyDocumento484 pagineAll HematologyIrene NgesaNessuna valutazione finora
- BloodDocumento6 pagineBloodBell GatesNessuna valutazione finora
- Anemia SDocumento42 pagineAnemia SCristinaGheorgheNessuna valutazione finora
- Hematology Notes for Medical StudentsDa EverandHematology Notes for Medical StudentsValutazione: 5 su 5 stelle5/5 (1)
- Takaful Health2Documento34 pagineTakaful Health2yusofprubsnNessuna valutazione finora
- Gangguan Hemodinamik, Trombosis Dan Syok: Fk-Uncen JayapuraDocumento67 pagineGangguan Hemodinamik, Trombosis Dan Syok: Fk-Uncen Jayapuramarsal25Nessuna valutazione finora
- Giger and DavidhizarDocumento4 pagineGiger and DavidhizarHv EstokNessuna valutazione finora
- Nutritional Status of Filipino Pre-School Children (2-5 Years Old)Documento20 pagineNutritional Status of Filipino Pre-School Children (2-5 Years Old)Car OrdzNessuna valutazione finora
- Ebulletin IAP Nov 2017Documento57 pagineEbulletin IAP Nov 2017pediatric servicesNessuna valutazione finora
- International Classification of Sleep Disorders: Third EditionDocumento5 pagineInternational Classification of Sleep Disorders: Third Editiongruukgruuk0% (1)
- Fernandez ED101 Module 2 PDFDocumento28 pagineFernandez ED101 Module 2 PDFChristine ElnasNessuna valutazione finora
- 300+ TOP CASE MANAGER Objective Questions and AnswersDocumento29 pagine300+ TOP CASE MANAGER Objective Questions and AnswersHANEESH JOHNNessuna valutazione finora
- Heat Exhaustion DehydrationDocumento3 pagineHeat Exhaustion Dehydrationnoor amirullahNessuna valutazione finora
- Effects of Alcohol, Tobacco, and Marijuana - PR 1Documento11 pagineEffects of Alcohol, Tobacco, and Marijuana - PR 1Mark Andris GempisawNessuna valutazione finora
- ‘Topical Application of Avena Sativa in Managing Uremic Xerosis, Hyperpigmentation, and Pruritus among Patients with Chronic Kidney Disease: A Comprehensive Review’ Leeba L J1 , Smitha P V2 , Usharani E NDocumento9 pagine‘Topical Application of Avena Sativa in Managing Uremic Xerosis, Hyperpigmentation, and Pruritus among Patients with Chronic Kidney Disease: A Comprehensive Review’ Leeba L J1 , Smitha P V2 , Usharani E NeditorbijnrNessuna valutazione finora
- HOMOEOPATHY Tips and SecretsDocumento814 pagineHOMOEOPATHY Tips and SecretsrajeshwaridhabadheNessuna valutazione finora
- Analytical ExpositionDocumento2 pagineAnalytical ExpositionIva Titin ShoviaNessuna valutazione finora
- Neurological DisordersDocumento10 pagineNeurological DisorderssoumenNessuna valutazione finora
- Development and Content Validity of A Website ForDocumento7 pagineDevelopment and Content Validity of A Website Forrickelme.businessNessuna valutazione finora
- Patient Profile: 1 - PageDocumento6 paginePatient Profile: 1 - PageRoane RoblesNessuna valutazione finora
- PDF History Physical Examination Laboratorytesting and Emergency Department DDDocumento17 paginePDF History Physical Examination Laboratorytesting and Emergency Department DDNurul FatimahNessuna valutazione finora
- English Iii For Nursing Student: Unit 3 AdmissionDocumento4 pagineEnglish Iii For Nursing Student: Unit 3 Admissiongriesna wheniNessuna valutazione finora
- Case Study - CharleinDocumento13 pagineCase Study - Charleinmacky_lumberaNessuna valutazione finora
- Novel Drug Approvals For 2022 FDADocumento3 pagineNovel Drug Approvals For 2022 FDAGeorge ZachariahNessuna valutazione finora
- Cardiovascular EngineeringDocumento257 pagineCardiovascular EngineeringSeyit Hamza ÇavgaNessuna valutazione finora
- CHCPAL001 Student Assessment Booklet - AGE (ID 98478)Documento49 pagineCHCPAL001 Student Assessment Booklet - AGE (ID 98478)Francis Dave Peralta Bitong50% (2)
- Oral SurgeryDocumento40 pagineOral Surgeryshekinah echavezNessuna valutazione finora
- Immunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthDocumento92 pagineImmunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthPolychase Magaoay100% (1)
- Assessment 011 1Documento11 pagineAssessment 011 1ManawNessuna valutazione finora
- Environmental Streptococci and Enterococcus Spp. - A Practical Summary For Controlling Mastitis - VirginiaAg DASC-7P (2012)Documento2 pagineEnvironmental Streptococci and Enterococcus Spp. - A Practical Summary For Controlling Mastitis - VirginiaAg DASC-7P (2012)userNessuna valutazione finora
- Csec Human and Social Biology Syllabus OutlineDocumento3 pagineCsec Human and Social Biology Syllabus OutlineCHRISTOPHER SCALENessuna valutazione finora
- Chemistry ProjectDocumento18 pagineChemistry Projectishana KhanNessuna valutazione finora