Potrebbero piacerti anche
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3Da EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3Nessuna valutazione finora
- 5 Cases FungalDocumento56 pagine5 Cases Fungalkoteshwara raoNessuna valutazione finora
- Venous Thromboembolism (VTE) Prophylaxis inDocumento24 pagineVenous Thromboembolism (VTE) Prophylaxis inVesna EfremNessuna valutazione finora
- Labor Room Managementduring Covid19-5Documento78 pagineLabor Room Managementduring Covid19-5Kalyani RathNessuna valutazione finora
- Labuang Baji Hospital, Tuesday, June 27th, 2023 (Period June 21th-June 25th, 2023) - DTDocumento3 pagineLabuang Baji Hospital, Tuesday, June 27th, 2023 (Period June 21th-June 25th, 2023) - DTradhiah karimNessuna valutazione finora
- Uganda - Advanced HIV Disease - Screening ToolDocumento47 pagineUganda - Advanced HIV Disease - Screening Toolithran khoNessuna valutazione finora
- 7 Cases FungalDocumento56 pagine7 Cases Fungalkoteshwara raoNessuna valutazione finora
- 4a Study - Diagnostic SW-1Documento36 pagine4a Study - Diagnostic SW-1LELLYNessuna valutazione finora
- Epid 600 Class 8 BiasDocumento51 pagineEpid 600 Class 8 BiasRobinNessuna valutazione finora
- Normal Spontaneous Vagina Delivery: Group 11: Case PresentationDocumento9 pagineNormal Spontaneous Vagina Delivery: Group 11: Case PresentationMikes CastroNessuna valutazione finora
- Perina IAN 28.09.2020 FinDocumento10 paginePerina IAN 28.09.2020 FinRyan IlhamNessuna valutazione finora
- Clustering Data Sheet and Concept Map and Nursing Care Plan PosteopreativeDocumento4 pagineClustering Data Sheet and Concept Map and Nursing Care Plan PosteopreativeAyman NabilNessuna valutazione finora
- pch13221 PDFDocumento4 paginepch13221 PDFshine8395Nessuna valutazione finora
- Testing For HIV Infection in Pregnancy: P S (ID 2008-02)Documento4 pagineTesting For HIV Infection in Pregnancy: P S (ID 2008-02)shine8395Nessuna valutazione finora
- Nbsmanual 28 6 2015 160712064159 PDFDocumento86 pagineNbsmanual 28 6 2015 160712064159 PDFDIMAMIANessuna valutazione finora
- Zisovska-SCORING SYSTEMS IN NEONATOLOGYDocumento45 pagineZisovska-SCORING SYSTEMS IN NEONATOLOGYrahermd1971Nessuna valutazione finora
- Emergency Obstetric and NEWBORN CARE: The DOH Protocol: National Safe Motherhood Program BY:Department of HealthDocumento35 pagineEmergency Obstetric and NEWBORN CARE: The DOH Protocol: National Safe Motherhood Program BY:Department of HealthAlexander Miguel M. AbasNessuna valutazione finora
- G Covid 19Documento19 pagineG Covid 19Nabilla Sophia SofyanNessuna valutazione finora
- Assessment and Management Women in PregnantDocumento1 paginaAssessment and Management Women in Pregnantanisah tri agustiniNessuna valutazione finora
- Screening For Congenital and Developmental DisordersDocumento20 pagineScreening For Congenital and Developmental DisordersEricNessuna valutazione finora
- Ob-Gyn For The Generalist: International Patient Safety Goals (IPSG)Documento8 pagineOb-Gyn For The Generalist: International Patient Safety Goals (IPSG)carmsNessuna valutazione finora
- MFM Guidance For COVID-19: Table 1Documento5 pagineMFM Guidance For COVID-19: Table 1Phaniraj RamachandrulaNessuna valutazione finora
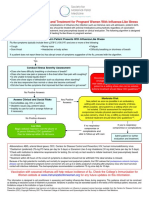
- 2017 Influenza AlgorithmDocumento1 pagina2017 Influenza AlgorithmFrandita Ivana TanisiwaNessuna valutazione finora
- Duty Report RIWDocumento41 pagineDuty Report RIWRiyan W. PratamaNessuna valutazione finora
- Cburbachcareplan 2Documento8 pagineCburbachcareplan 2api-520843051Nessuna valutazione finora
- COVID 19 AlgorithmDocumento1 paginaCOVID 19 AlgorithmSonia Capirosi AyuningtiasNessuna valutazione finora
- Surgery PearlsDocumento2 pagineSurgery Pearlspatriciaatan1497Nessuna valutazione finora
- Clinical Pathway DengueDocumento4 pagineClinical Pathway Denguedr. Albertus S.ANessuna valutazione finora
- Maternity Care For Mothers and Babies During The COVID-19 PandemicDocumento33 pagineMaternity Care For Mothers and Babies During The COVID-19 PandemicAllyssa Joy Orajay PeraltaNessuna valutazione finora
- Daftar Tilik Ketrampilan Klinik Penjahitan PerineumDocumento54 pagineDaftar Tilik Ketrampilan Klinik Penjahitan PerineumRyan IlhamNessuna valutazione finora
- G JaundiceDocumento40 pagineG JaundiceRedina Tuya RamirezNessuna valutazione finora
- Junio Covid-19 - Sanford GuideDocumento8 pagineJunio Covid-19 - Sanford GuideEfraín Castilla MinayaNessuna valutazione finora
- Neonatal Jaundice PathwayDocumento35 pagineNeonatal Jaundice Pathwaypragita ayu100% (1)
- Sample Case Studies of COVID-19 in PregnancyDocumento29 pagineSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNessuna valutazione finora
- SA04 Medical Examination Report PDFDocumento4 pagineSA04 Medical Examination Report PDFSOU FEI Ang0% (1)
- Enhanced Influenzalike Illness Community Survei Llance Severe Acure Respiratory Infection Surveillance Referal Flow and ResponseDocumento4 pagineEnhanced Influenzalike Illness Community Survei Llance Severe Acure Respiratory Infection Surveillance Referal Flow and ResponseVanessa EdizaNessuna valutazione finora
- Pathology Ultrasound Ordering by RMRNNPDocumento27 paginePathology Ultrasound Ordering by RMRNNPAbeer MohammedNessuna valutazione finora
- Tele Visit For COVID Testing Today If Patient Meets Criteria For Testing Order 87635 Covid-19 Poc AMBDocumento2 pagineTele Visit For COVID Testing Today If Patient Meets Criteria For Testing Order 87635 Covid-19 Poc AMBShrutiNessuna valutazione finora
- Nursing Care 2Documento1 paginaNursing Care 2Moh. H.AlObaidyNessuna valutazione finora
- English Patient Screening Form 19Documento1 paginaEnglish Patient Screening Form 19Armando VillaNessuna valutazione finora
- IMNCI2021Documento94 pagineIMNCI2021Let BNessuna valutazione finora
- STEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsDocumento2 pagineSTEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsahjkseflhasefNessuna valutazione finora
- Pre e Learning PlanDocumento14 paginePre e Learning Planapi-555538380Nessuna valutazione finora
- Moderna (Health Declaration Screening Form) Eng - June 18 2021Documento1 paginaModerna (Health Declaration Screening Form) Eng - June 18 2021Paulo Justin Tabangcora OropillaNessuna valutazione finora
- MSA in STIDocumento36 pagineMSA in STISuhazeli Abdullah100% (2)
- Trichomoniasis and Bacterial Vaginosis in Pregnancy: Inadequately Managed With The Syndromic ApproachDocumento10 pagineTrichomoniasis and Bacterial Vaginosis in Pregnancy: Inadequately Managed With The Syndromic ApproachIqra AnugerahNessuna valutazione finora
- Antenatal TestingDocumento7 pagineAntenatal TestingSherri O'BrienNessuna valutazione finora
- Critical Appraisal Cross Sectional Case ControlDocumento76 pagineCritical Appraisal Cross Sectional Case ControlAndita SyabanaNessuna valutazione finora
- Patients Health Screening Form 1Documento1 paginaPatients Health Screening Form 1dennis buclanNessuna valutazione finora
- Wiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroDocumento35 pagineWiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroIfah Inayah D'zatrichaNessuna valutazione finora
- Dialysis Inovative Facility Policies and ProceduresDocumento3 pagineDialysis Inovative Facility Policies and ProceduresFrancis Marven Lee LocsinNessuna valutazione finora
- Application Iii ChnlecDocumento2 pagineApplication Iii ChnlecAiwon Zeihane FloresNessuna valutazione finora
- Name D.O.B Collection No Treating Physician Sex Collection Date Molecular BiologyDocumento1 paginaName D.O.B Collection No Treating Physician Sex Collection Date Molecular BiologyIBJOMERNessuna valutazione finora
- Journal Report FinalDocumento33 pagineJournal Report FinalKevin Marcial AralarNessuna valutazione finora
- Assessment of A Pregnant FamilyDocumento4 pagineAssessment of A Pregnant FamilyLuna Sang-anNessuna valutazione finora
- Preseptal and Orbital Cellulitis in Children Clinical Guideline V4.0 June 2021Documento12 paginePreseptal and Orbital Cellulitis in Children Clinical Guideline V4.0 June 2021Exo L1485Nessuna valutazione finora
- Humanimmunodeficiency Virusinitialassessmentand Routinefollow-UpDocumento16 pagineHumanimmunodeficiency Virusinitialassessmentand Routinefollow-UpBriando Stevano LinelejanNessuna valutazione finora
- UntitledDocumento20 pagineUntitledFatma OmaraNessuna valutazione finora
- Pelvic Inflammatory Disease (PID)Documento16 paginePelvic Inflammatory Disease (PID)CHRISTIAN RAY ALPAS PASILIAONessuna valutazione finora
- 2.04 Surgical Illness in PregnancyDocumento6 pagine2.04 Surgical Illness in PregnancyRaquel ReyesNessuna valutazione finora
- Racial Disparities in Postpartum Pain Management.4Documento7 pagineRacial Disparities in Postpartum Pain Management.4piano543Nessuna valutazione finora
- Oral Board Crib Memory PDFDocumento10 pagineOral Board Crib Memory PDFpiano543Nessuna valutazione finora
- 12 in 12Documento1 pagina12 in 12piano543Nessuna valutazione finora
- 06 SMI Nifedipine Algorithm July 2017Documento1 pagina06 SMI Nifedipine Algorithm July 2017piano543Nessuna valutazione finora
- 03 SMI Eclampsia Checklist July 2017Documento1 pagina03 SMI Eclampsia Checklist July 2017piano543100% (1)
- Name of My Service: Please Call (555) 555-1234 or Text (555) 555-5678Documento2 pagineName of My Service: Please Call (555) 555-1234 or Text (555) 555-5678piano543Nessuna valutazione finora
- PAA Neighborhood Survey 2016Documento11 paginePAA Neighborhood Survey 2016piano543Nessuna valutazione finora
- Mock Oral Series LegendDocumento1 paginaMock Oral Series Legendpiano543Nessuna valutazione finora
- Mock Oral Exams IDocumento28 pagineMock Oral Exams Ipiano543Nessuna valutazione finora
- Ultrasound BasicsDocumento2 pagineUltrasound Basicspiano543Nessuna valutazione finora
- Sia Breathe MeDocumento7 pagineSia Breathe MeEnrico VolpatoNessuna valutazione finora
- 1996 Ite ExamDocumento72 pagine1996 Ite Exampiano543Nessuna valutazione finora
- Anesthesia Drugs Quick Reference Low ResDocumento6 pagineAnesthesia Drugs Quick Reference Low Respiano543Nessuna valutazione finora
- Remote Access Portal User Guide SSLVPNDocumento11 pagineRemote Access Portal User Guide SSLVPNpiano543Nessuna valutazione finora
- Aldrete Discharge ScoresDocumento1 paginaAldrete Discharge Scorespiano543Nessuna valutazione finora
- Medtext 2007 A-Type QuestionsDocumento16 pagineMedtext 2007 A-Type Questionspiano543Nessuna valutazione finora
- FA Mnemonics JSDocumento7 pagineFA Mnemonics JSpiano543Nessuna valutazione finora
- Introduction of The Topic: Nano-BiotechnologyDocumento7 pagineIntroduction of The Topic: Nano-BiotechnologyAbhishek YadavNessuna valutazione finora
- DNA and ChromosomeDocumento15 pagineDNA and ChromosomeYudha OkpriandaNessuna valutazione finora
- Diseases of The CallitrichidaeDocumento48 pagineDiseases of The CallitrichidaeCristhian HernandezNessuna valutazione finora
- Ultimate Guide To Surviving in The WildDocumento175 pagineUltimate Guide To Surviving in The WildSal Ot100% (1)
- Day Cream: Material Safety Data SheetDocumento2 pagineDay Cream: Material Safety Data SheetRachmawati AfridaNessuna valutazione finora
- Aliphatic and Aromatic HydrocarbonsDocumento13 pagineAliphatic and Aromatic HydrocarbonsdhaineyNessuna valutazione finora
- Clinical Manual of OtolaryngologyDocumento49 pagineClinical Manual of Otolaryngologygamecockusc1992100% (3)
- Dorothea Orem: Self-Care TheoryDocumento16 pagineDorothea Orem: Self-Care TheoryHazel LezahNessuna valutazione finora
- Multiple Dengue Virus Types Harbored by Individual MosquitoesDocumento7 pagineMultiple Dengue Virus Types Harbored by Individual MosquitoesYL Slalu BahagieaNessuna valutazione finora
- AyyDocumento187 pagineAyyZoé WolfesNessuna valutazione finora
- OME Video DurationsDocumento7 pagineOME Video DurationsLucas RiosNessuna valutazione finora
- Ob Osce.04 CTG ReadingDocumento6 pagineOb Osce.04 CTG ReadingDasha VeeNessuna valutazione finora
- How To Implement Health Technology Assessment - 230715 - 093605Documento10 pagineHow To Implement Health Technology Assessment - 230715 - 093605Nour ElsabahNessuna valutazione finora
- Design Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukDocumento33 pagineDesign Theory: Boo Virk Simon Andrews Boo - Virk@babraham - Ac.uk Simon - Andrews@babraham - Ac.ukuzma munirNessuna valutazione finora
- Cor Pulmonale PATHOPHYSIOLOGYDocumento2 pagineCor Pulmonale PATHOPHYSIOLOGYChloie Marie RosalejosNessuna valutazione finora
- Neurology & Pupils (No 467)Documento231 pagineNeurology & Pupils (No 467)Mohamed GaberNessuna valutazione finora
- Accupressure EyeDocumento7 pagineAccupressure Eyemayxanh1234100% (3)
- PhysiologyDocumento31 paginePhysiologyraza20100% (1)
- DMC FinalsDocumento64 pagineDMC Finalskaye agustinNessuna valutazione finora
- Lesson Plan in Science Perpetuation of Life I. Learning ObjectivesDocumento3 pagineLesson Plan in Science Perpetuation of Life I. Learning ObjectivesRachel Lorenzo SaldoNessuna valutazione finora
- At Merienda - Individual ActivityDocumento6 pagineAt Merienda - Individual ActivityMoreno, John Gil F.Nessuna valutazione finora
- Varicose Vein and Its Homeopathic Cure - DR Bashir Mahmud ElliasDocumento8 pagineVaricose Vein and Its Homeopathic Cure - DR Bashir Mahmud ElliasBashir Mahmud Ellias100% (2)
- Nature and Characteristics of Services in HospitalsDocumento7 pagineNature and Characteristics of Services in HospitalsOun MuhammadNessuna valutazione finora
- The Validity of Acupuncture in Veterinary MedicineDocumento10 pagineThe Validity of Acupuncture in Veterinary MedicinePaolaNessuna valutazione finora
- Multi-Disease Prediction With Machine LearningDocumento7 pagineMulti-Disease Prediction With Machine LearningUmar KhanNessuna valutazione finora
- Colic in Horse: A Presentation OnDocumento32 pagineColic in Horse: A Presentation OnMuhammad Saif KhanNessuna valutazione finora
- Feed Additives, Antibodies, Poultry Vaccines 2023.3Documento6 pagineFeed Additives, Antibodies, Poultry Vaccines 2023.3Bruce YangNessuna valutazione finora
- Burning Mouth Syndrome 1Documento16 pagineBurning Mouth Syndrome 1Mihika BalaNessuna valutazione finora
- John Medina - Brain Rules PDFDocumento11 pagineJohn Medina - Brain Rules PDFDiego Cunha100% (2)
- Guide For Writing NotesDocumento10 pagineGuide For Writing Notesiamsera100% (1)