Potrebbero piacerti anche
- P ' R O R N 2008: Etiology/EpidemiologyDocumento10 pagineP ' R O R N 2008: Etiology/EpidemiologyDiana MitreaNessuna valutazione finora
- P ' R O R N 2008: Etiology/EpidemiologyDocumento10 pagineP ' R O R N 2008: Etiology/EpidemiologyDiana MitreaNessuna valutazione finora
- GCT in Males by Dr. Musaib MushtaqDocumento44 pagineGCT in Males by Dr. Musaib MushtaqDr. Musaib MushtaqNessuna valutazione finora
- 13 Recent Advances in Management of Hodhkin's LymphomaDocumento63 pagine13 Recent Advances in Management of Hodhkin's LymphomaVipul BansalNessuna valutazione finora
- P ' R O R N 2008: Etiology/EpidemiologyDocumento10 pagineP ' R O R N 2008: Etiology/EpidemiologyDiana MitreaNessuna valutazione finora
- Clinical Oncology: Marigold D.R. Majarucon-Ferrolino MD, FPCP, FpsmoDocumento186 pagineClinical Oncology: Marigold D.R. Majarucon-Ferrolino MD, FPCP, FpsmoWaiwit KritayakiranaNessuna valutazione finora
- Gastriccancer 160428190410Documento54 pagineGastriccancer 160428190410Pranavi ShewaleNessuna valutazione finora
- Gestational Trophoblastic Disease Pt2Documento75 pagineGestational Trophoblastic Disease Pt2yurie_ameliaNessuna valutazione finora
- 1 - Hodgkin's LymphomaDocumento12 pagine1 - Hodgkin's LymphomaDiana MitreaNessuna valutazione finora
- Bladdercancerabeerfinal 170701110656Documento94 pagineBladdercancerabeerfinal 170701110656Aravindh SharmaNessuna valutazione finora
- UrooncologyDocumento49 pagineUrooncologyanwar jabariNessuna valutazione finora
- Pathology: Human PapillomavirusDocumento15 paginePathology: Human Papillomavirussandeepv08Nessuna valutazione finora
- Gis 1 EnglishDocumento85 pagineGis 1 Englishexand861Nessuna valutazione finora
- Lung Cancer Lecture Notes (Quick Summary)Documento4 pagineLung Cancer Lecture Notes (Quick Summary)Ibrahim FoondunNessuna valutazione finora
- Medullary CancerDocumento32 pagineMedullary CancerLily DenekeNessuna valutazione finora
- What Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistDocumento26 pagineWhat Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistjehemirNessuna valutazione finora
- Presented By: Moderator: Dr. Vikas KumarDocumento104 paginePresented By: Moderator: Dr. Vikas KumarWorku KifleNessuna valutazione finora
- 3 - Pediatric Wilms' TumorDocumento5 pagine3 - Pediatric Wilms' TumorDiana MitreaNessuna valutazione finora
- Astro 2015 Refresher Head NeckDocumento175 pagineAstro 2015 Refresher Head Necknova agustaNessuna valutazione finora
- 陳v Endometrial Cancer 2Documento48 pagine陳v Endometrial Cancer 201范芷紜Nessuna valutazione finora
- Angelic - Doc - Breast CancerDocumento12 pagineAngelic - Doc - Breast CancerAngy100% (2)
- Testicular TumorsDocumento42 pagineTesticular TumorsarhamNessuna valutazione finora
- Breast CancerDocumento62 pagineBreast CancerChris Jardine LiNessuna valutazione finora
- Testicular Tumours - Mashaal SaadDocumento26 pagineTesticular Tumours - Mashaal Saadshahryar shaukatNessuna valutazione finora
- Anal CancerDocumento2 pagineAnal CancerRamez AntakiaNessuna valutazione finora
- Small Cell Lung Cancer: Osama Elzaafarany, MDDocumento38 pagineSmall Cell Lung Cancer: Osama Elzaafarany, MDaandakuNessuna valutazione finora
- Thyroid CancerDocumento28 pagineThyroid CancerIoana CozmaNessuna valutazione finora
- Ovarian CA 450918 SHDocumento52 pagineOvarian CA 450918 SH180045Nessuna valutazione finora
- Ugi GistDocumento10 pagineUgi Gistian3yeung-2Nessuna valutazione finora
- Management of Throid CancerDocumento65 pagineManagement of Throid Cancerد.صلاح مبروك خلافNessuna valutazione finora
- Optimizing The Management of NSCLCDocumento34 pagineOptimizing The Management of NSCLCANISA RACHMITA ARIANTI 2020Nessuna valutazione finora
- Carcinoma Uterus - Amita MaheshwariDocumento42 pagineCarcinoma Uterus - Amita MaheshwariMochammad Rizal AttamimiNessuna valutazione finora
- Radio Therapeutic and Oncological Treatment of Cancer of TheDocumento21 pagineRadio Therapeutic and Oncological Treatment of Cancer of Theayodeji78Nessuna valutazione finora
- Anal Canal CarcinomaDocumento24 pagineAnal Canal CarcinomaArun guruNessuna valutazione finora
- Advances in Surgery-LrrcDocumento62 pagineAdvances in Surgery-LrrcHarshit SrivastavaNessuna valutazione finora
- Nancy Gastric CancerDocumento36 pagineNancy Gastric Cancernancy voraNessuna valutazione finora
- Management of Endometrial CarcinomaDocumento46 pagineManagement of Endometrial CarcinomaSapna SNessuna valutazione finora
- The Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Documento165 pagineThe Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Bianca DanielaNessuna valutazione finora
- Golden Rules in OncologyDocumento76 pagineGolden Rules in OncologyDragonNessuna valutazione finora
- Carcinoma Thyroid: Diagnosis and Management: Professor Ravi KantDocumento51 pagineCarcinoma Thyroid: Diagnosis and Management: Professor Ravi KantMubarakDiedaNessuna valutazione finora
- Ann Oncol 2011 Aebi Vi12 24Documento13 pagineAnn Oncol 2011 Aebi Vi12 24Yipno Wanhar El MawardiNessuna valutazione finora
- Thyroid Cancer Case Discussion by DR Salah MabroukDocumento38 pagineThyroid Cancer Case Discussion by DR Salah MabroukDr. Salah Mabrouk KhalafNessuna valutazione finora
- Treatment of Breast Cancer: DR - Syed Alam ZebDocumento51 pagineTreatment of Breast Cancer: DR - Syed Alam ZebSucipto HartonoNessuna valutazione finora
- Surgery Bladder TumorDocumento35 pagineSurgery Bladder TumorMuhammad ArsalNessuna valutazione finora
- Powerpoint: Breast CancerDocumento89 paginePowerpoint: Breast Cancerj.doe.hex_8780% (5)
- Laryngeal Cancer: Anh Q. Truong MS-4 University of Washington, SOMDocumento33 pagineLaryngeal Cancer: Anh Q. Truong MS-4 University of Washington, SOMSri Agustina0% (1)
- Role of Radiotherapy For Hepatocellular CarcinomaDocumento37 pagineRole of Radiotherapy For Hepatocellular CarcinomabahtiarhabibiNessuna valutazione finora
- Carcinoma CervixDocumento45 pagineCarcinoma CervixDhananjaya ShivalingappaNessuna valutazione finora
- Breast TreatmentDocumento6 pagineBreast TreatmentzainabNessuna valutazione finora
- Testicular CancerDocumento48 pagineTesticular Cancerluckyswiss7776848Nessuna valutazione finora
- Guide Lines For Management of Prostate CancerDocumento37 pagineGuide Lines For Management of Prostate CancerPuneet SethNessuna valutazione finora
- Thyroid CancerDocumento11 pagineThyroid Cancerreem.khafagyyNessuna valutazione finora
- Update On Thyroid NodulesDocumento57 pagineUpdate On Thyroid NodulesHarshit SrivastavaNessuna valutazione finora
- Malignant MelanomaDocumento31 pagineMalignant MelanomakityamuwesiNessuna valutazione finora
- Thyroid CancerDocumento38 pagineThyroid CancersarahNessuna valutazione finora
- Curriculum Vitae: Lulus Handayani, MDDocumento31 pagineCurriculum Vitae: Lulus Handayani, MDpisangphoeNessuna valutazione finora
- Management of Testicular Neoplasms: DR - Suresh Babu Final Yr - PG Prof - Dr.Shanmugam M.S. Unit 3Documento44 pagineManagement of Testicular Neoplasms: DR - Suresh Babu Final Yr - PG Prof - Dr.Shanmugam M.S. Unit 3Aarthi BalaNessuna valutazione finora
- Ata Guidelines SeminarDocumento49 pagineAta Guidelines SeminarArnab KalitaNessuna valutazione finora
- Cases Surgery For Non-Melanoma Skin Cancers: bcc, scc, mcc.Da EverandCases Surgery For Non-Melanoma Skin Cancers: bcc, scc, mcc.Nessuna valutazione finora
- Neuroendocrine Tumors: Surgical Evaluation and ManagementDa EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNessuna valutazione finora
- RTQA Prescription WorksheetDocumento6 pagineRTQA Prescription WorksheetDiana MitreaNessuna valutazione finora
- How To Evaluate The Scientific Evidence and Apply It To Daily PracticeDocumento2 pagineHow To Evaluate The Scientific Evidence and Apply It To Daily PracticeDiana MitreaNessuna valutazione finora
- Ncologist: Imaging in Radiation Oncology: A PerspectiveDocumento12 pagineNcologist: Imaging in Radiation Oncology: A PerspectiveDiana MitreaNessuna valutazione finora
- Piis0167814014005246 PDFDocumento8 paginePiis0167814014005246 PDFDiana MitreaNessuna valutazione finora
- 2 - Low Grade GliomaDocumento5 pagine2 - Low Grade GliomaDiana MitreaNessuna valutazione finora
- 3 - Pediatric Wilms' TumorDocumento5 pagine3 - Pediatric Wilms' TumorDiana MitreaNessuna valutazione finora
- 4 - Clinical EpidemiologyDocumento8 pagine4 - Clinical EpidemiologyDiana Mitrea100% (1)
- Technical Innovations & Patient Support in Radiation OncologyDocumento9 pagineTechnical Innovations & Patient Support in Radiation OncologyDiana MitreaNessuna valutazione finora
- Colon - Icd-O C18 - 19Documento6 pagineColon - Icd-O C18 - 19Diana MitreaNessuna valutazione finora
- 4 Radiobiology of Brachytherapy and The Dose-Rate EffectDocumento27 pagine4 Radiobiology of Brachytherapy and The Dose-Rate EffectDiana MitreaNessuna valutazione finora
- P ' R O R N 2008: Epidemiology/EtiologyDocumento17 pagineP ' R O R N 2008: Epidemiology/EtiologyDiana MitreaNessuna valutazione finora
- 1 - Benign DiseaseDocumento5 pagine1 - Benign DiseaseDiana MitreaNessuna valutazione finora
- 1 - Hodgkin's LymphomaDocumento12 pagine1 - Hodgkin's LymphomaDiana MitreaNessuna valutazione finora
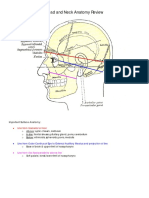
- 1 - Head and Neck Anatomy Review LiteDocumento34 pagine1 - Head and Neck Anatomy Review LiteDiana MitreaNessuna valutazione finora
- Cheat Sheet - Melkman & GreenDocumento2 pagineCheat Sheet - Melkman & GreenDiana MitreaNessuna valutazione finora
- Registration: 29° Residential Course Modern Radiotherapy, Time Issues and New DrugsDocumento1 paginaRegistration: 29° Residential Course Modern Radiotherapy, Time Issues and New DrugsDiana MitreaNessuna valutazione finora
- 1 - Breast Cancer ReviewDocumento26 pagine1 - Breast Cancer ReviewDiana MitreaNessuna valutazione finora
- B CellDocumento291 pagineB CellDiana Mitrea0% (1)
- 2up NCCNTB BreastDocumento38 pagine2up NCCNTB BreastDiana MitreaNessuna valutazione finora
- Stupidity of Human Race. Be Thankful For ThatDocumento1 paginaStupidity of Human Race. Be Thankful For ThatDiana MitreaNessuna valutazione finora
- Bla Bla BlaDocumento1 paginaBla Bla BlaDiana MitreaNessuna valutazione finora
- Puritan Bennett 980 Ventilator Clinical Applications Lesson Plan PresentationDocumento102 paginePuritan Bennett 980 Ventilator Clinical Applications Lesson Plan Presentationbilal ahmad100% (1)
- Fucicort CreamDocumento4 pagineFucicort Creamcupcake xNessuna valutazione finora
- T2 Nandayapa AlejandraDocumento2 pagineT2 Nandayapa AlejandraNandayapa Santana AlejandraNessuna valutazione finora
- TURP SyndromeDocumento13 pagineTURP SyndromeWindy Ari WijayaNessuna valutazione finora
- Chapter 12 - Urinary SystemDocumento50 pagineChapter 12 - Urinary SystemynaNessuna valutazione finora
- Warming Up: 1. Discuss in Your Class: (Write Your Own Answers. Points Only Given For Reference)Documento8 pagineWarming Up: 1. Discuss in Your Class: (Write Your Own Answers. Points Only Given For Reference)FOXTROTNessuna valutazione finora
- Acko-Download-802 230116 105832Documento5 pagineAcko-Download-802 230116 105832RichiNessuna valutazione finora
- Small Animal DermatologyDocumento278 pagineSmall Animal DermatologyManuel Rodriguez100% (1)
- Mammography Solutions: Serenys Serenys DR Serenys DBTDocumento4 pagineMammography Solutions: Serenys Serenys DR Serenys DBTHanna FettahNessuna valutazione finora
- Mantoux Test FactsheetDocumento6 pagineMantoux Test FactsheetMuhammad FikrieNessuna valutazione finora
- NCP Module 5Documento2 pagineNCP Module 5Kathleen AngNessuna valutazione finora
- Wounds and Other Injuries PDFDocumento30 pagineWounds and Other Injuries PDFRhonda BushNessuna valutazione finora
- Anaerobic InfectionsDocumento36 pagineAnaerobic InfectionsPatriceNessuna valutazione finora
- Module 6 Drug EducationDocumento84 pagineModule 6 Drug EducationAnn Margaret BalajadiaNessuna valutazione finora
- General Diet MelDocumento125 pagineGeneral Diet MelWen SilverNessuna valutazione finora
- Sheet 1Documento30 pagineSheet 1ahmed amiraliNessuna valutazione finora
- Pil 15213Documento14 paginePil 15213Vinayaka.P.V 202Nessuna valutazione finora
- Case Study 4Documento9 pagineCase Study 4DIANE GRACE CUEVAS MIGUEL100% (1)
- Case ReportDocumento6 pagineCase ReportJoshua Diaz QuiquijanaNessuna valutazione finora
- Consent Form For Oral SurgeryWisdom Teeth RemovalDocumento2 pagineConsent Form For Oral SurgeryWisdom Teeth RemovalNishtha Kumar0% (1)
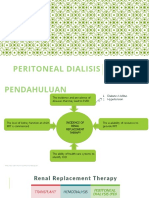
- DT Peritoneal Dialysis DektaDocumento21 pagineDT Peritoneal Dialysis Dektailham nugrohoNessuna valutazione finora
- ALERGIADocumento50 pagineALERGIADiana IoanaNessuna valutazione finora
- Special Circumstances Guidelines ALSDocumento19 pagineSpecial Circumstances Guidelines ALSHamzaMasoodNessuna valutazione finora
- 2023new Heart Failure Guidelines Impact On The Patient Journey The Healthcare Professional PerspectiDocumento53 pagine2023new Heart Failure Guidelines Impact On The Patient Journey The Healthcare Professional PerspectimarianacavenaghiNessuna valutazione finora
- Is Calcium Phosphate Augmentation A Viable Option For Osteoporotic Hip Fractures?Documento8 pagineIs Calcium Phosphate Augmentation A Viable Option For Osteoporotic Hip Fractures?Santiago MartinezNessuna valutazione finora
- Management Severe DengueDocumento18 pagineManagement Severe DengueMuhammad Fhandeka IsrarNessuna valutazione finora
- COVID-19 InterimGuidelines Treatment ENGDocumento25 pagineCOVID-19 InterimGuidelines Treatment ENGMartin PaturlanneNessuna valutazione finora
- Clinical SignificanceDocumento3 pagineClinical Significanceapi-539267574Nessuna valutazione finora
- 285-Article Text-631-1-10-20191002Documento6 pagine285-Article Text-631-1-10-20191002Claudia BuheliNessuna valutazione finora