Potrebbero piacerti anche
- Ayurvedic HerbsDocumento19 pagineAyurvedic HerbsAlejandra GuerreroNessuna valutazione finora
- Best Homeopathic Medicine For BradycardiaDocumento9 pagineBest Homeopathic Medicine For BradycardiaAlamgirNessuna valutazione finora
- Shen-Atlas of AcupunctureDocumento256 pagineShen-Atlas of AcupunctureMiguel A Cordero100% (1)
- Final Death Note - Compre NotesDocumento1.550 pagineFinal Death Note - Compre NotesSteph TabasaNessuna valutazione finora
- Respiratory Disorders: Parainfluenza, RSV, RhinovirusDocumento5 pagineRespiratory Disorders: Parainfluenza, RSV, RhinovirusSoojung Nam100% (1)
- Respiratory System-Review PathoDocumento100 pagineRespiratory System-Review PathoSadiePartington-RiopelleNessuna valutazione finora
- Sepia OfficinalisDocumento30 pagineSepia OfficinalisDebosmito Nayek100% (1)
- Breath Sounds: ConsiderationsDocumento10 pagineBreath Sounds: ConsiderationsKarl RobleNessuna valutazione finora
- Disorder of Respiratory SystemDocumento89 pagineDisorder of Respiratory SystemDarine NasrNessuna valutazione finora
- Assessing and Managing Respiratory DistressDocumento3 pagineAssessing and Managing Respiratory DistressGen RodriguezNessuna valutazione finora
- Ineffective Airway ClearanceDocumento2 pagineIneffective Airway ClearanceHanya Bint PotawanNessuna valutazione finora
- Bates Thorax Lungs With TermsDocumento4 pagineBates Thorax Lungs With Termscrystalshe100% (1)
- CoughDocumento30 pagineCoughAnil NarayanNessuna valutazione finora
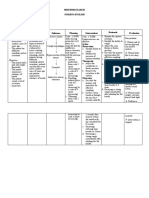
- NCPDocumento9 pagineNCPEjie Boy Isaga67% (3)
- Nursing Interventions for Ineffective Airway ClearanceDocumento3 pagineNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- Causes and Possible Prevention of Asthma and AllergiesDa EverandCauses and Possible Prevention of Asthma and AllergiesNessuna valutazione finora
- Lung Cancer Presentation: DR Richard Sullivan and Ms Anne FraserDocumento24 pagineLung Cancer Presentation: DR Richard Sullivan and Ms Anne FraseranggiNessuna valutazione finora
- A & B Materia Medica by AlphabetDocumento46 pagineA & B Materia Medica by AlphabetYASIR KHAN100% (2)
- Respiratory System AssessmentDocumento13 pagineRespiratory System Assessmentavinash dhameriyaNessuna valutazione finora
- Pulmonary SystemDocumento75 paginePulmonary Systemangeles_robert_71Nessuna valutazione finora
- Daftar Obat Prekursor & OOTDocumento2 pagineDaftar Obat Prekursor & OOTMinul1412Nessuna valutazione finora
- Bronchial AsthmaDocumento71 pagineBronchial AsthmaHero MondaresNessuna valutazione finora
- Child With Respiratory DysfunctionDocumento23 pagineChild With Respiratory DysfunctionmeganNessuna valutazione finora
- RespiratoryDocumento34 pagineRespiratoryanasokour100% (1)
- Bronchial Asthma: Harun ElçiçekDocumento54 pagineBronchial Asthma: Harun ElçiçekFiras Ali100% (2)
- MCN CompiledDocumento71 pagineMCN CompiledJœnríčk AzueloNessuna valutazione finora
- Thorax and Lungs ReferenceDocumento8 pagineThorax and Lungs Referencegwynth ripaldaNessuna valutazione finora
- Respiratory SystemDocumento2 pagineRespiratory SystemJ MNessuna valutazione finora
- Cough لاعس ہفرس۔ یسناھک TussisDocumento4 pagineCough لاعس ہفرس۔ یسناھک TussisSulthana Rasiya NNessuna valutazione finora
- Lung Sounds Guide: Vesicular, Bronchial, Crackles & MoreDocumento24 pagineLung Sounds Guide: Vesicular, Bronchial, Crackles & MoreAswinNessuna valutazione finora
- 1.) Anatomy and Physiology of The Respiratory SystemDocumento6 pagine1.) Anatomy and Physiology of The Respiratory SystemFaith SarmientoNessuna valutazione finora
- Lung Auscultation Sounds GuideDocumento3 pagineLung Auscultation Sounds GuideCristina TofanNessuna valutazione finora
- The Thorax and Lungs - BATESDocumento4 pagineThe Thorax and Lungs - BATESsitalcoolk100% (2)
- Chapter 27Documento6 pagineChapter 27monster40lbsNessuna valutazione finora
- Jordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryDocumento11 pagineJordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryJordan Abosama MamalumpongNessuna valutazione finora
- Physiological Overview in Relation To PracticeDocumento52 paginePhysiological Overview in Relation To PracticedrkhaledassemNessuna valutazione finora
- Diseases of The Respiratory System Diseases of The Respiratory System Principles of Respiratory InsufficiencyDocumento9 pagineDiseases of The Respiratory System Diseases of The Respiratory System Principles of Respiratory InsufficiencyJaafar AlzuheiriNessuna valutazione finora
- Lung Examination: AbnormalDocumento56 pagineLung Examination: AbnormalBECAREFUL89ANessuna valutazione finora
- Human Respiratory SystemDocumento4 pagineHuman Respiratory Systemno nameNessuna valutazione finora
- Examination of Respiratory SystemDocumento78 pagineExamination of Respiratory Systemwidya sri hastutiNessuna valutazione finora
- Term For Slow and Deep Breathing With Regular RhythmDocumento2 pagineTerm For Slow and Deep Breathing With Regular RhythmDave MarimonNessuna valutazione finora
- Lower Respiratory Disorders Part 1Documento70 pagineLower Respiratory Disorders Part 1Joseph Krafft100% (1)
- Rev Widya Physical Examination of Respiratory SystemDocumento72 pagineRev Widya Physical Examination of Respiratory SystemYuliaNessuna valutazione finora
- Child With CoughDocumento59 pagineChild With CoughAdekunle JosephNessuna valutazione finora
- NOTES2Documento7 pagineNOTES2Angelica BautistaNessuna valutazione finora
- Name: Jake Yvan G. Dizon Year Level: BSN IIIDocumento2 pagineName: Jake Yvan G. Dizon Year Level: BSN IIIJake Yvan DizonNessuna valutazione finora
- Respiratory SoundsDocumento2 pagineRespiratory SoundsMuhammad NaeemjakNessuna valutazione finora
- Respiratory Assessment & DiagnosticsDocumento9 pagineRespiratory Assessment & DiagnosticsAngellene GraceNessuna valutazione finora
- Reviewer For Management of Common IllnessDocumento27 pagineReviewer For Management of Common Illnessmarie vennis hamchawanNessuna valutazione finora
- Respiratory System Bullet PointsDocumento5 pagineRespiratory System Bullet PointsArun KumarNessuna valutazione finora
- Oxygenation 1Documento155 pagineOxygenation 1Khatlen BagaresNessuna valutazione finora
- 2300 - Module 4 - Basic Respiratory PathophysiologyDocumento26 pagine2300 - Module 4 - Basic Respiratory Pathophysiologymegan.abbinkNessuna valutazione finora
- Breathing SoundsDocumento3 pagineBreathing Soundsalthea jade villadonga100% (1)
- Thorax and LungsDocumento11 pagineThorax and LungsJoel SantosNessuna valutazione finora
- Anatomi Fisiologi Sistem Pernafasan - Id.enDocumento7 pagineAnatomi Fisiologi Sistem Pernafasan - Id.enCindy Ari SantiNessuna valutazione finora
- Cough: by Dr. Meghana Patil (Intern Batch 2016)Documento24 pagineCough: by Dr. Meghana Patil (Intern Batch 2016)Meghana PatilNessuna valutazione finora
- Pulmonary Examination - Knowledge at AMBOSSDocumento1 paginaPulmonary Examination - Knowledge at AMBOSSKC Dela RosaNessuna valutazione finora
- Patho Respiratory - KatherineDocumento9 paginePatho Respiratory - KatherineKayla MayerNessuna valutazione finora
- Case 3 - Anatomy and Physiology - SalimbagatDocumento4 pagineCase 3 - Anatomy and Physiology - SalimbagatChristine Pialan SalimbagatNessuna valutazione finora
- Healing 1 - Respiratory SystemDocumento9 pagineHealing 1 - Respiratory SystemErika Dela CruzNessuna valutazione finora
- Cough PBLDocumento3 pagineCough PBLDella FerginaNessuna valutazione finora
- Lung AuscultationDocumento62 pagineLung AuscultationOlea CroitorNessuna valutazione finora
- Respiratory SystemDocumento85 pagineRespiratory SystemDr:-Ustaad Aakass Ahmed Junejo SahabNessuna valutazione finora
- 1-The Respiratory SystemDocumento7 pagine1-The Respiratory SystemEma FröhlichováNessuna valutazione finora
- Grade 9 Science Respirstory SystemDocumento35 pagineGrade 9 Science Respirstory SystemMark Anthony ClavillasNessuna valutazione finora
- Lung ExaminationDocumento14 pagineLung Examinationსალომე მუმლაძე “Slay” TMANessuna valutazione finora
- IPPADocumento4 pagineIPPAIsaac KipchumbaNessuna valutazione finora
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocumento7 pagineNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNessuna valutazione finora
- Assessmentpulmonary 151014090912 Lva1 App6892Documento63 pagineAssessmentpulmonary 151014090912 Lva1 App6892sasNessuna valutazione finora
- The Respiratory SystemDocumento8 pagineThe Respiratory SystemJane Rose SuperadaNessuna valutazione finora
- ENT LectureDocumento14 pagineENT Lectureمنى حاج احمد100% (1)
- Respiratory SystemDocumento82 pagineRespiratory Systemsubhojitnayek100% (2)
- The Respiratory System: Gas Exchange and AnatomyDocumento8 pagineThe Respiratory System: Gas Exchange and AnatomyTriza AndradeNessuna valutazione finora
- Depression, Anxiety and Stress Among Nursing Students in Sri LankaDocumento13 pagineDepression, Anxiety and Stress Among Nursing Students in Sri LankaJœnríčk AzueloNessuna valutazione finora
- Acute Care and Emergency General Surgery in Patients With Chronic Liver Disease: How Can We Optimize Perioperative Care? A Review of The LiteratureDocumento9 pagineAcute Care and Emergency General Surgery in Patients With Chronic Liver Disease: How Can We Optimize Perioperative Care? A Review of The LiteratureJœnríčk AzueloNessuna valutazione finora
- Toxoplasmosis: Bishara J. Freij, MD and John L. Sever, MD, PHDFDocumento12 pagineToxoplasmosis: Bishara J. Freij, MD and John L. Sever, MD, PHDFJœnríčk AzueloNessuna valutazione finora
- Disorders: By: Nur Hanisah Binti ZainorenDocumento53 pagineDisorders: By: Nur Hanisah Binti ZainorenJœnríčk AzueloNessuna valutazione finora
- Chapter 52. Nursing Care of The Child With A Traumatic Injury TermsDocumento8 pagineChapter 52. Nursing Care of The Child With A Traumatic Injury TermsJœnríčk AzueloNessuna valutazione finora
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocumento1 paginaChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Nursing Care for Children with Musculoskeletal DisordersDocumento3 pagineNursing Care for Children with Musculoskeletal DisordersJœnríčk AzueloNessuna valutazione finora
- Chapter 42. Nursing Care of The Child With An Immune Disorder TermsDocumento2 pagineChapter 42. Nursing Care of The Child With An Immune Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Administering Eye Medication MaterialsDocumento1 paginaAdministering Eye Medication MaterialsJœnríčk AzueloNessuna valutazione finora
- Nursing Care of Children with Hematologic DisordersDocumento8 pagineNursing Care of Children with Hematologic DisordersJœnríčk AzueloNessuna valutazione finora
- IMCI GuidelinesDocumento173 pagineIMCI Guidelineskabamba0% (1)
- Nursing Care of Children with Cardiovascular DisordersDocumento11 pagineNursing Care of Children with Cardiovascular DisordersJœnríčk AzueloNessuna valutazione finora
- WATER SANITATION Group 1 CHN LEC SECTION BDocumento7 pagineWATER SANITATION Group 1 CHN LEC SECTION BJœnríčk AzueloNessuna valutazione finora
- Rationale 14 18Documento2 pagineRationale 14 18Jœnríčk AzueloNessuna valutazione finora
- Rationale For 16 30Documento2 pagineRationale For 16 30Jœnríčk AzueloNessuna valutazione finora
- Chapter 40 ADocumento4 pagineChapter 40 AJœnríčk AzueloNessuna valutazione finora
- Child Urinary Tract Infection Case StudyDocumento10 pagineChild Urinary Tract Infection Case StudyJœnríčk AzueloNessuna valutazione finora
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocumento1 paginaChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Mask Patterns PDFDocumento1 paginaMask Patterns PDFJœnríčk AzueloNessuna valutazione finora
- Written Activity For CHN Instructions 1Documento3 pagineWritten Activity For CHN Instructions 1Jœnríčk AzueloNessuna valutazione finora
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocumento1 paginaChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Chapter 42. Nursing Care of The Child With An Immune Disorder TermsDocumento2 pagineChapter 42. Nursing Care of The Child With An Immune Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Nursing Care of Children with Cardiovascular DisordersDocumento11 pagineNursing Care of Children with Cardiovascular DisordersJœnríčk AzueloNessuna valutazione finora
- Chapter 40 ADocumento4 pagineChapter 40 AJœnríčk AzueloNessuna valutazione finora
- Nursing Care of Children with Cardiovascular DisordersDocumento11 pagineNursing Care of Children with Cardiovascular DisordersJœnríčk AzueloNessuna valutazione finora
- Chapter 42. Nursing Care of The Child With An Immune Disorder TermsDocumento2 pagineChapter 42. Nursing Care of The Child With An Immune Disorder TermsJœnríčk AzueloNessuna valutazione finora
- Treating Perineal Infection with Guava LeavesDocumento2 pagineTreating Perineal Infection with Guava LeavesJœnríčk AzueloNessuna valutazione finora
- Situation 15. The Community Health Nurse Prepares/participate in The Preparation of TheDocumento3 pagineSituation 15. The Community Health Nurse Prepares/participate in The Preparation of TheJœnríčk AzueloNessuna valutazione finora
- Aetiology: Obe, FFCM, F.FQMDocumento5 pagineAetiology: Obe, FFCM, F.FQMYusfi RydokaNessuna valutazione finora
- 10 Communicable DiseasesDocumento3 pagine10 Communicable DiseasesPauline de VeraNessuna valutazione finora
- Absen Metod!!!Documento4 pagineAbsen Metod!!!Haris Pratama RebornNessuna valutazione finora
- COVID in Children - AdvisoryDocumento2 pagineCOVID in Children - AdvisorySMN CV APPLICATIONSNessuna valutazione finora
- Dhudhi Badi ImportantDocumento4 pagineDhudhi Badi ImportantpoonamNessuna valutazione finora
- Problem Oriented Medical Record: Mr. S/ 74 yo/ERDocumento7 pagineProblem Oriented Medical Record: Mr. S/ 74 yo/ERDitra TryasniansaNessuna valutazione finora
- Textbook of Respiratory Disease in Dogs and Cats Acute and Chronic CoughDocumento5 pagineTextbook of Respiratory Disease in Dogs and Cats Acute and Chronic CoughDiego CushicóndorNessuna valutazione finora
- MIDTERM EXAM III NURSING ENGLISHDocumento3 pagineMIDTERM EXAM III NURSING ENGLISHAlfriedo 008Nessuna valutazione finora
- Farmacopia Fall Immunity Builder GuideDocumento56 pagineFarmacopia Fall Immunity Builder GuideddNessuna valutazione finora
- 5-Febtelegram2019 Correct by New GroupDocumento24 pagine5-Febtelegram2019 Correct by New GroupFammo MoiduNessuna valutazione finora
- Rudraksha (Elaeocarpus Ganitrus) Benefits & UsesDocumento16 pagineRudraksha (Elaeocarpus Ganitrus) Benefits & UsesSuresh S.RNessuna valutazione finora
- Clinical Case Study Presentation - MJDocumento37 pagineClinical Case Study Presentation - MJapi-365372933Nessuna valutazione finora
- Liceo de Cagayan University: Chili Pepper (Capsicum Frutescens) As Chocolate CandyDocumento33 pagineLiceo de Cagayan University: Chili Pepper (Capsicum Frutescens) As Chocolate CandyRaven EscabusaNessuna valutazione finora
- CA - Adult Health Nursing PDFDocumento55 pagineCA - Adult Health Nursing PDFMarvin Heramis RyanNessuna valutazione finora
- A Detailed Lesson Plan in Living Things and Their Environment (Respiratory and Circulatory System: Relation)Documento22 pagineA Detailed Lesson Plan in Living Things and Their Environment (Respiratory and Circulatory System: Relation)Don LaguismaNessuna valutazione finora
- NaHSO3 Natrium BisulfitDocumento6 pagineNaHSO3 Natrium BisulfitAnyberta Dwi ListyantiNessuna valutazione finora
- Cough: - Atheer AljthalinDocumento15 pagineCough: - Atheer AljthalinAmira AlmutairiNessuna valutazione finora