Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Association of Antioxidant Enzymes and MDA Level in Diabetic Nephropathy Patients in Indore Region of Madhya PradeshDocumento6 pagineAssociation of Antioxidant Enzymes and MDA Level in Diabetic Nephropathy Patients in Indore Region of Madhya PradeshAriNessuna valutazione finora
- Review Article Oxidative Stress As The Main Target in Diabetic Retinopathy PathophysiologyDocumento22 pagineReview Article Oxidative Stress As The Main Target in Diabetic Retinopathy PathophysiologyAriNessuna valutazione finora
- Review Article: Oxidative Stress in MyopiaDocumento13 pagineReview Article: Oxidative Stress in MyopiaAriNessuna valutazione finora
- 10.1016/j.bbadis.2015.08.001: BBA - Molecular Basis of DiseaseDocumento48 pagine10.1016/j.bbadis.2015.08.001: BBA - Molecular Basis of DiseaseAriNessuna valutazione finora
- 10 3389@fphys 2020 00463 PDFDocumento10 pagine10 3389@fphys 2020 00463 PDFAriNessuna valutazione finora
- Jurnal Esotropia 3Documento5 pagineJurnal Esotropia 3AriNessuna valutazione finora
- Jurnal EsotropiaDocumento5 pagineJurnal EsotropiaAriNessuna valutazione finora
- Ciprofloxaxin Endoph PDFDocumento1 paginaCiprofloxaxin Endoph PDFAriNessuna valutazione finora
- Kortikosteroid EndofDocumento5 pagineKortikosteroid EndofAriNessuna valutazione finora
- HHS Public Access: Pitfalls in The Use of Stereoacuity in The Diagnosis of Non-Organic Visual LossDocumento13 pagineHHS Public Access: Pitfalls in The Use of Stereoacuity in The Diagnosis of Non-Organic Visual LossAriNessuna valutazione finora
- Slit LampDocumento2 pagineSlit LampAriNessuna valutazione finora
- Corneal LayerDocumento9 pagineCorneal LayerAriNessuna valutazione finora
- FUNDUSCOPY and SEGMENT ANTERIOR DRAWINGDocumento12 pagineFUNDUSCOPY and SEGMENT ANTERIOR DRAWINGAriNessuna valutazione finora
- 1 SMDocumento7 pagine1 SMAriNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
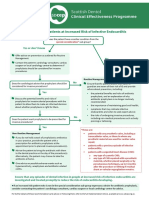
- SDCEP Antibiotic Prophylaxis Summary FlowchartDocumento1 paginaSDCEP Antibiotic Prophylaxis Summary FlowchartMahmoud EladawyNessuna valutazione finora
- Tiny Earth ReportDocumento3 pagineTiny Earth ReportJordan CastleberryNessuna valutazione finora
- Antitussive and Antibacterial Activity of Trompang Elepante (Heliotropium Indicum Linn.)Documento5 pagineAntitussive and Antibacterial Activity of Trompang Elepante (Heliotropium Indicum Linn.)Neust TrainingNessuna valutazione finora
- Current and Future Prospects For Nanotechnology in Animal ProductionDocumento13 pagineCurrent and Future Prospects For Nanotechnology in Animal ProductionDr. Adnan Al-KanaanNessuna valutazione finora
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocumento2 pagineDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNessuna valutazione finora
- Kamala KannanDocumento103 pagineKamala KannanshrikantNessuna valutazione finora
- Diseases Caused by MicroorganismsDocumento9 pagineDiseases Caused by MicroorganismsKhushbuGuptaNessuna valutazione finora
- Repeat Breeding in Cattle and BuffaloesDocumento34 pagineRepeat Breeding in Cattle and BuffaloesGovind Narayan Purohit100% (2)
- Evaluation of Phytochemical and Antimicrobial Activity of Achyranthus AsperaDocumento4 pagineEvaluation of Phytochemical and Antimicrobial Activity of Achyranthus AsperaInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Drug StudyDocumento4 pagineDrug StudyMelvin D. RamosNessuna valutazione finora
- Reading New E2 PDFDocumento50 pagineReading New E2 PDFMary Jis100% (1)
- Synthesis of Silver Nanoparticles: Ahmed Mostafa HusseinDocumento76 pagineSynthesis of Silver Nanoparticles: Ahmed Mostafa Husseinjenny joseNessuna valutazione finora
- Brine Shrimp Lethality Assay of The Ethanolic Extracts of Three Selected Species of Medicinal Plants From Iligan City, PhilippinesDocumento4 pagineBrine Shrimp Lethality Assay of The Ethanolic Extracts of Three Selected Species of Medicinal Plants From Iligan City, PhilippinesMustafizur Rahman AviNessuna valutazione finora
- MicrobiologyDocumento2 pagineMicrobiologyLovely SarangiNessuna valutazione finora
- Analysis Of Molecular Docking Quersetin, Guaijavarin And MORIN-3-O-Α-L-Arabopyranoside As AntibacterialDocumento9 pagineAnalysis Of Molecular Docking Quersetin, Guaijavarin And MORIN-3-O-Α-L-Arabopyranoside As AntibacterialRaisaNessuna valutazione finora
- Implementation and Use of Point of Care C R 2022 Journal of The American MedDocumento11 pagineImplementation and Use of Point of Care C R 2022 Journal of The American MedPuttryNessuna valutazione finora
- Antibiotic Mcqs June 04Documento6 pagineAntibiotic Mcqs June 04Mirza GhalibNessuna valutazione finora
- A Comparative Study of Antibacterial Activity of Leaves and Latex of Jatropha Curcas LDocumento5 pagineA Comparative Study of Antibacterial Activity of Leaves and Latex of Jatropha Curcas Lanna luthfiahNessuna valutazione finora
- Caring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyDocumento34 pagineCaring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyRubinaNessuna valutazione finora
- Evmlu Uganda.2020Documento124 pagineEvmlu Uganda.2020ALINOMUGASHA EMMANUELNessuna valutazione finora
- Bab 1 Biologi Umum 1 - UGM - Pengantar Dan Materi Penyusun MHDocumento56 pagineBab 1 Biologi Umum 1 - UGM - Pengantar Dan Materi Penyusun MHulfi lathifahNessuna valutazione finora
- Book 3Documento431 pagineBook 3ms msNessuna valutazione finora
- 1 OnlineDocumento6 pagine1 Onlineanalisaapil312Nessuna valutazione finora
- Journal Club 1Documento2 pagineJournal Club 1api-549451092Nessuna valutazione finora
- Clostridium Difficile Guideline - UMMCDocumento5 pagineClostridium Difficile Guideline - UMMCdamondouglas100% (3)
- Microorganisms: Friends and FoeDocumento32 pagineMicroorganisms: Friends and FoePROYASH ASSAM100% (1)
- Micropara-Lab c5-c7Documento10 pagineMicropara-Lab c5-c7Monica JoyceNessuna valutazione finora
- Module 4-VMED 5335Documento28 pagineModule 4-VMED 5335PETJSNVENessuna valutazione finora
- Bronchopneumonia JurnalDocumento8 pagineBronchopneumonia JurnalMuhd AfizyNessuna valutazione finora
- Lakatan Banana As Antibacterial SoapDocumento5 pagineLakatan Banana As Antibacterial SoapJames JonasNessuna valutazione finora