Potrebbero piacerti anche
- EFT GuideDocumento11 pagineEFT Guidenokaion19% (26)
- FWA CMS Training (4346) PDFDocumento13 pagineFWA CMS Training (4346) PDFinfo3497Nessuna valutazione finora
- Hazard Analysis in The WorkplaceDocumento7 pagineHazard Analysis in The WorkplaceUghlahnNessuna valutazione finora
- Pathology Intro Part 1 PDFDocumento13 paginePathology Intro Part 1 PDFAmy LalringhluaniNessuna valutazione finora
- Students Sleep During Classes: The Amount of Time VariesDocumento7 pagineStudents Sleep During Classes: The Amount of Time Variesjason_aaNessuna valutazione finora
- IGCSE Biology (O610) Workbook: Balanced DietDocumento5 pagineIGCSE Biology (O610) Workbook: Balanced DietPatrick Abidra100% (1)
- Competency Based Training Programme: Guidelines ForDocumento42 pagineCompetency Based Training Programme: Guidelines ForPrithwiraj MaitiNessuna valutazione finora
- Competency Based Training Programme: Guidelines ForDocumento42 pagineCompetency Based Training Programme: Guidelines ForPrithwiraj MaitiNessuna valutazione finora
- Competency Based Training Programme: Guidelines ForDocumento42 pagineCompetency Based Training Programme: Guidelines ForPrithwiraj MaitiNessuna valutazione finora
- Bacterial Sepsis: I. The Concept of SepsisDocumento8 pagineBacterial Sepsis: I. The Concept of SepsisIsra BalyNessuna valutazione finora
- Physiological Changes Postpartum PeriodDocumento2 paginePhysiological Changes Postpartum PeriodEurielle MioleNessuna valutazione finora
- Emergency Medicine CurriculumDocumento29 pagineEmergency Medicine Curriculumdhiran showriNessuna valutazione finora
- Fast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaDa EverandFast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaNessuna valutazione finora
- Recurrent MeningitisDocumento14 pagineRecurrent Meningitisidno1008Nessuna valutazione finora
- Case Study Neonatal SepsisDocumento24 pagineCase Study Neonatal Sepsisreiche90% (29)
- I14 FullDocumento9 pagineI14 FullJoseph Brima SambaNessuna valutazione finora
- Nej MR A 2026131Documento19 pagineNej MR A 2026131Juan JoseNessuna valutazione finora
- 10 Cytokine StormDocumento19 pagine10 Cytokine StormAndres Felipe Hurtado BautistaNessuna valutazione finora
- Suptipos de SepsisDocumento17 pagineSuptipos de SepsisoswaldoninaNessuna valutazione finora
- Antibiotics and Palliative CareDocumento6 pagineAntibiotics and Palliative CareRahmanu ReztaputraNessuna valutazione finora
- Grunewald 2019Documento22 pagineGrunewald 2019Josver PretellNessuna valutazione finora
- Igg 4Documento12 pagineIgg 4emmanuel AndemNessuna valutazione finora
- Diagnostic Approach To Chronic MeningitisDocumento19 pagineDiagnostic Approach To Chronic MeningitisJuan P. RuedaNessuna valutazione finora
- Megacolon Toxic of Idiophatic Origin: Case ReportDocumento6 pagineMegacolon Toxic of Idiophatic Origin: Case ReportgayutNessuna valutazione finora
- Artigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanDocumento4 pagineArtigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanRENATA SANTOS ASSUNCAONessuna valutazione finora
- SarcoidosisDocumento22 pagineSarcoidosisveerraju tvNessuna valutazione finora
- 1 s2.0 S0749070421001019 MainDocumento17 pagine1 s2.0 S0749070421001019 MainEliseu AmaralNessuna valutazione finora
- Case Studies: Episodic Fever and Neutropenia in A 22-Year-Old MaleDocumento5 pagineCase Studies: Episodic Fever and Neutropenia in A 22-Year-Old MaleCindy Yunuen LeónNessuna valutazione finora
- 2018 Inflammageing Chronic Inflammation in Ageing, Cardiovascular Disease, and FrailtyDocumento39 pagine2018 Inflammageing Chronic Inflammation in Ageing, Cardiovascular Disease, and FrailtyJuanPablo Pino GonzalezNessuna valutazione finora
- Prolonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanDocumento6 pagineProlonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanFerdy AlviandoNessuna valutazione finora
- Systemic - Sclerosis Nature Review 2014Documento22 pagineSystemic - Sclerosis Nature Review 2014CT TANNessuna valutazione finora
- Neutropenia and Febrile Neutropenia-1Documento42 pagineNeutropenia and Febrile Neutropenia-1safia ahmedNessuna valutazione finora
- Primer: Systemic SclerosisDocumento21 paginePrimer: Systemic Sclerosishumberto_620Nessuna valutazione finora
- The Diagnostic Role of PCT and Other Biomarkers in Discriminating Infectious From Non-Infectious FeverDocumento8 pagineThe Diagnostic Role of PCT and Other Biomarkers in Discriminating Infectious From Non-Infectious Fevergwyneth.green.512Nessuna valutazione finora
- Emerging Therapies in Chronic Spontaneous UrticariaDocumento12 pagineEmerging Therapies in Chronic Spontaneous UrticariaComité Alergólogos InmunólogosNessuna valutazione finora
- Non Neoplastic WBC DisordersDocumento13 pagineNon Neoplastic WBC DisordersSheikh UzairNessuna valutazione finora
- Nyarang'o Dennis Level IIIDocumento29 pagineNyarang'o Dennis Level IIIBryan AmataNessuna valutazione finora
- Manejo Meningitis Art 2022 IngDocumento5 pagineManejo Meningitis Art 2022 Ingroman rodriguezNessuna valutazione finora
- Bacterial Meningitis Patho PaperDocumento5 pagineBacterial Meningitis Patho PaperJessica BrayNessuna valutazione finora
- Langerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesDocumento4 pagineLangerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesYuniita VerayantiiNessuna valutazione finora
- Ofy 038Documento5 pagineOfy 038Rosandi AdamNessuna valutazione finora
- Transverse Myelitis: Clinical PracticeDocumento9 pagineTransverse Myelitis: Clinical PracticearnabNessuna valutazione finora
- Management of HemophagocyticDocumento10 pagineManagement of HemophagocyticAlexander CanoNessuna valutazione finora
- Journal Reading Morbus HansenDocumento29 pagineJournal Reading Morbus HansenyoantamaraNessuna valutazione finora
- L. Ari Jutkowitz, VMD, DACVECC Michigan State University East Lansing, MI, USADocumento5 pagineL. Ari Jutkowitz, VMD, DACVECC Michigan State University East Lansing, MI, USAyoedanuxNessuna valutazione finora
- Staphy 2Documento5 pagineStaphy 2Alexandra MariaNessuna valutazione finora
- Arpa - 2018 0219 RaDocumento6 pagineArpa - 2018 0219 Rahuseikha velayazulfahdNessuna valutazione finora
- Non Neoplastic WBC DisordersDocumento17 pagineNon Neoplastic WBC Disordersdr100% (1)
- Idsa GuidelinesDocumento34 pagineIdsa GuidelinesROSEN NNessuna valutazione finora
- Third Case Report Pseudomembranous Colitis Dr. Lisa FarianiDocumento18 pagineThird Case Report Pseudomembranous Colitis Dr. Lisa FarianirizkyauliautamaNessuna valutazione finora
- IDSA Nec FascDocumento34 pagineIDSA Nec FascShameen KhanNessuna valutazione finora
- 2023, FranzenDocumento14 pagine2023, FranzenAlexandra TofanNessuna valutazione finora
- Manifestaciones Extrahepaticas Hepatitis CDocumento15 pagineManifestaciones Extrahepaticas Hepatitis CSMIBA MedicinaNessuna valutazione finora
- Epidemic Cerebrospinal MeningitisDocumento49 pagineEpidemic Cerebrospinal MeningitisDrAbhilash RMNessuna valutazione finora
- Cytokine Storm and Leukocyte Changes in Mild Versus SevereDocumento25 pagineCytokine Storm and Leukocyte Changes in Mild Versus SevereRaffaharianggaraNessuna valutazione finora
- Babesiosis in Pregnancy: An Imitator of HELLP SyndromeDocumento6 pagineBabesiosis in Pregnancy: An Imitator of HELLP Syndromemade dharmaNessuna valutazione finora
- Kikuchi's Disease: Malathi Sathiyasekaran R. Varadharajan So. ShivbalanDocumento3 pagineKikuchi's Disease: Malathi Sathiyasekaran R. Varadharajan So. Shivbalanzulfikar adiNessuna valutazione finora
- TuberculomaDocumento4 pagineTuberculomalittlecandiesNessuna valutazione finora
- DR Julian-MYOCARDITISDocumento83 pagineDR Julian-MYOCARDITISArmando Esteban Coa SandovalNessuna valutazione finora
- Dermatomyositis Case7Documento15 pagineDermatomyositis Case7Hanina Macataman MetmugNessuna valutazione finora
- Adult Still's Disease and Respiratory Failure in A 74 Year Old WomanDocumento3 pagineAdult Still's Disease and Respiratory Failure in A 74 Year Old WomanEduardo Romero StéfaniNessuna valutazione finora
- Walter H. Maloney, M.DDocumento6 pagineWalter H. Maloney, M.DIvan DarioNessuna valutazione finora
- Lecture-3.3.6-Systemic Autoimmune Diseases With Examples-2Documento3 pagineLecture-3.3.6-Systemic Autoimmune Diseases With Examples-2aditya sahuNessuna valutazione finora
- An Atypical Presentation of Kikuchi-Fujimoto Disease Mimicking Systemic Lupus Erythematosus: Case Report and Literature ReviewDocumento5 pagineAn Atypical Presentation of Kikuchi-Fujimoto Disease Mimicking Systemic Lupus Erythematosus: Case Report and Literature Reviewzulfikar adiNessuna valutazione finora
- Cureus 0015 00000038234Documento8 pagineCureus 0015 00000038234Anggita Nara SafitriNessuna valutazione finora
- Running Head: CASE STUDY PAPER 1Documento14 pagineRunning Head: CASE STUDY PAPER 1Issaiah Nicolle CeciliaNessuna valutazione finora
- Pseudomembranouse ColitisDocumento37 paginePseudomembranouse ColitisFitria FieraNessuna valutazione finora
- Unusual Cause of Fever in A 35-Year-Old Man: ECP YuenDocumento4 pagineUnusual Cause of Fever in A 35-Year-Old Man: ECP YuenhlNessuna valutazione finora
- Laboratory Tests Confirming The Infection-Bahan BacaanDocumento3 pagineLaboratory Tests Confirming The Infection-Bahan Bacaanelroy badkissNessuna valutazione finora
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumDa EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNessuna valutazione finora
- Sops On Covid-19 Vaccination of Persons Without Prescribed Identity Cards Through CowinDocumento3 pagineSops On Covid-19 Vaccination of Persons Without Prescribed Identity Cards Through CowinKuthuraikaranNessuna valutazione finora
- CasesDocumento6 pagineCasesram11221Nessuna valutazione finora
- New SN of Polling Station Locality Building in Which It Will Be Polling Areas Wheather For All Voters or Men Only or Women OnlyDocumento51 pagineNew SN of Polling Station Locality Building in Which It Will Be Polling Areas Wheather For All Voters or Men Only or Women OnlyJugal HarkutNessuna valutazione finora
- List of Judicial OfficersDocumento1 paginaList of Judicial OfficersJugal HarkutNessuna valutazione finora
- DM CCMDocumento20 pagineDM CCMAbhyuday KumarNessuna valutazione finora
- Neurosurgery - Spinal Trauma - WB Animation Transcript - Richard FoxDocumento2 pagineNeurosurgery - Spinal Trauma - WB Animation Transcript - Richard FoxJugal HarkutNessuna valutazione finora
- Natboard-Data Publicnotice Notice 202107235847Documento1 paginaNatboard-Data Publicnotice Notice 202107235847LataNessuna valutazione finora
- Evidence Base of Clinical DiagnosisDocumento4 pagineEvidence Base of Clinical DiagnosisJugal HarkutNessuna valutazione finora
- B07DDHXNNSDocumento13 pagineB07DDHXNNSJugal HarkutNessuna valutazione finora
- B Type Natriuretic Peptide VHD Magne PDFDocumento24 pagineB Type Natriuretic Peptide VHD Magne PDFJugal HarkutNessuna valutazione finora
- Anti CD20 Monoclonal Antibodies Reviewing A RevolutionDocumento23 pagineAnti CD20 Monoclonal Antibodies Reviewing A RevolutionJugal HarkutNessuna valutazione finora
- A Method of Teaching Clinical Problem Solving Skills To Primary Health Care Student NursesDocumento5 pagineA Method of Teaching Clinical Problem Solving Skills To Primary Health Care Student NursesJugal HarkutNessuna valutazione finora
- Hospital Pharmacy Communication - NewsletterDocumento5 pagineHospital Pharmacy Communication - Newsletterjuveria nausheenNessuna valutazione finora
- Covid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaDocumento6 pagineCovid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaIJAR JOURNALNessuna valutazione finora
- Drug Treatment of AnemiasDocumento29 pagineDrug Treatment of AnemiasKashmalaNessuna valutazione finora
- Calories Needed For A 17 Year Old, 70 KG MaleDocumento7 pagineCalories Needed For A 17 Year Old, 70 KG Maleboom boomNessuna valutazione finora
- Safety Pocket Guide Web 061808Documento534 pagineSafety Pocket Guide Web 061808hombre911100% (1)
- CephalosporinsDocumento20 pagineCephalosporinsBianca Andrea RagazaNessuna valutazione finora
- Coordination Group For Mutual Recognition and Decentralised Procedures - Human (CMDH)Documento12 pagineCoordination Group For Mutual Recognition and Decentralised Procedures - Human (CMDH)aslkdjNessuna valutazione finora
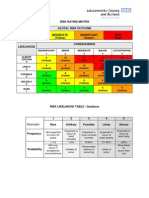
- Example of A NHS Risk Rating MatrixDocumento2 pagineExample of A NHS Risk Rating MatrixRochady SetiantoNessuna valutazione finora
- ERAS Protocols For Thyroid andDocumento9 pagineERAS Protocols For Thyroid andOskar MartinezNessuna valutazione finora
- Disaster Nursing SAS Session 14Documento6 pagineDisaster Nursing SAS Session 14Niceniadas CaraballeNessuna valutazione finora
- CVA StrokeDocumento6 pagineCVA StrokeMcrstna Lim SorianoNessuna valutazione finora
- Predicting and Controlling Influenza Outbreaks - Published Article - IJERSTE - Vol.12 Issue 2, Feb 2023Documento4 paginePredicting and Controlling Influenza Outbreaks - Published Article - IJERSTE - Vol.12 Issue 2, Feb 2023dimple kharwarNessuna valutazione finora
- Musculoskeletal Clinical Translation FrameworkDocumento1 paginaMusculoskeletal Clinical Translation FrameworkRafaelNessuna valutazione finora
- KEMH Guidelines On Cardiac Disease in PregnancyDocumento7 pagineKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaNessuna valutazione finora
- TheraDocumento4 pagineTheramaircusNessuna valutazione finora
- Health Declaration FormDocumento1 paginaHealth Declaration FormUzair KhalidNessuna valutazione finora
- Sarah J. (Englert) Dunham RN, BSN, MS, FNPDocumento3 pagineSarah J. (Englert) Dunham RN, BSN, MS, FNPapi-309264509Nessuna valutazione finora
- MOHAN Di. RAJU....... MOHAN Di. RAJU......Documento32 pagineMOHAN Di. RAJU....... MOHAN Di. RAJU......Nagaraja ReddyNessuna valutazione finora
- Prilosec (Omeprazole) MoreDocumento3 paginePrilosec (Omeprazole) MoreLuis Arturo Andrade CoronadoNessuna valutazione finora
- Esa Appeals FactsheetDocumento36 pagineEsa Appeals FactsheetClaire TNessuna valutazione finora
- Pediatric Blood Cancer - 2022 - Mader - Social Emotional and Behavioral Functioning in Young Childhood Cancer SurvivorsDocumento11 paginePediatric Blood Cancer - 2022 - Mader - Social Emotional and Behavioral Functioning in Young Childhood Cancer SurvivorsJuliana SoaresNessuna valutazione finora
- Lecture 1 Health, Safety & Environment (HSE)Documento23 pagineLecture 1 Health, Safety & Environment (HSE)A to z type videosNessuna valutazione finora
- Adani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalDocumento20 pagineAdani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalboxorNessuna valutazione finora
- State of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthDocumento228 pagineState of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthUNFPA SoWMYNessuna valutazione finora