Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Spelling Power Workbook PDFDocumento98 pagineSpelling Power Workbook PDFTinajazz100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Verb TensesDocumento3 pagineVerb TensesVeronicaGelfgren92% (12)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Module ConnectionsDocumento16 pagineModule ConnectionsHemilton Cheng Modulos100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Unit 2 Lab Manual ChemistryDocumento9 pagineUnit 2 Lab Manual ChemistryAldayne ParkesNessuna valutazione finora
- Determination of Royalty Rates For Trademarks and BrandsDocumento31 pagineDetermination of Royalty Rates For Trademarks and BrandsNicole EstefanieNessuna valutazione finora
- Plumbing - LecturesDocumento235 paginePlumbing - LecturesCirky NadleiNessuna valutazione finora
- Building Technology Preboard ExamDocumento4 pagineBuilding Technology Preboard Examkharen100% (1)
- Community Based Nutrition CMNPDocumento38 pagineCommunity Based Nutrition CMNPHamid Wafa100% (4)
- Complete ReviewerDocumento24 pagineComplete Reviewergene2693Nessuna valutazione finora
- MELSEC System Q: QJ71MES96 MES Interface ModuleDocumento364 pagineMELSEC System Q: QJ71MES96 MES Interface ModuleFajri AsyukronNessuna valutazione finora
- Digital Booklet - Halcyon (Deluxe)Documento7 pagineDigital Booklet - Halcyon (Deluxe)Renan LopesNessuna valutazione finora
- Compre Exam For Building TechnologyDocumento2 pagineCompre Exam For Building Technologygene2693100% (1)
- Petition For Bail Nonbailable LampaDocumento3 paginePetition For Bail Nonbailable LampaNikki MendozaNessuna valutazione finora
- Chapter 4 Lesson ProperDocumento44 pagineChapter 4 Lesson ProperWenceslao LynNessuna valutazione finora
- BCMSN30SG Vol.2 PDFDocumento394 pagineBCMSN30SG Vol.2 PDFShemariyahNessuna valutazione finora
- An/Trc - 170 TrainingDocumento264 pagineAn/Trc - 170 Trainingkapenrem2003Nessuna valutazione finora
- 1.06 Grouping of Ill Persons and Sources of DataDocumento2 pagine1.06 Grouping of Ill Persons and Sources of Datagene2693Nessuna valutazione finora
- 2.01 Measures of Disease FrequencyDocumento6 pagine2.01 Measures of Disease Frequencygene2693Nessuna valutazione finora
- 1.06 The Doctor-Doctor RelationshipDocumento3 pagine1.06 The Doctor-Doctor Relationshipgene2693Nessuna valutazione finora
- 1.04 The Medical ProfessionDocumento4 pagine1.04 The Medical Professiongene2693Nessuna valutazione finora
- 1.04 Strategies of EpidemiologyDocumento3 pagine1.04 Strategies of Epidemiologygene2693Nessuna valutazione finora
- 1.05 Descriptive Study DesignDocumento3 pagine1.05 Descriptive Study Designgene2693Nessuna valutazione finora
- Informed Consent: Maria Ana B. Mariano, MDDocumento4 pagineInformed Consent: Maria Ana B. Mariano, MDgene2693Nessuna valutazione finora
- Caticlan A1Documento1 paginaCaticlan A1gene2693Nessuna valutazione finora
- 1.03 Community Based Participatory ResearchDocumento2 pagine1.03 Community Based Participatory Researchgene2693Nessuna valutazione finora
- TermsDocumento1 paginaTermsgene2693Nessuna valutazione finora
- Operation Guide 5001: About This ManualDocumento3 pagineOperation Guide 5001: About This Manualgene2693Nessuna valutazione finora
- 1.02 Disease Causation PDFDocumento3 pagine1.02 Disease Causation PDFgene2693Nessuna valutazione finora
- 1.02 Physician Patient RelationshipDocumento5 pagine1.02 Physician Patient Relationshipgene2693Nessuna valutazione finora
- Principle of Design PDFDocumento54 paginePrinciple of Design PDFgene2693Nessuna valutazione finora
- PROPRACTT!Documento8 paginePROPRACTT!gene2693Nessuna valutazione finora
- Archt. Maundelito S. Florendo, UAP: The Brown BauhausDocumento12 pagineArcht. Maundelito S. Florendo, UAP: The Brown BauhausjrdolesinNessuna valutazione finora
- Online Shopping - Return FormDocumento1 paginaOnline Shopping - Return Formgene2693Nessuna valutazione finora
- Cost Estimate With LaborDocumento3 pagineCost Estimate With Laborgene2693Nessuna valutazione finora
- TheoryDocumento5 pagineTheoryRon GalitNessuna valutazione finora
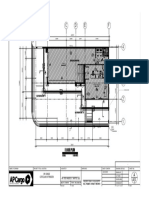
- Reflected Ceiling Plan: Ap Cargo Iligan BranchDocumento1 paginaReflected Ceiling Plan: Ap Cargo Iligan Branchgene2693Nessuna valutazione finora
- FAO Fisheries & Aquaculture - National Aquaculture Sector Overview - PhilippinesDocumento12 pagineFAO Fisheries & Aquaculture - National Aquaculture Sector Overview - Philippinesgene2693Nessuna valutazione finora
- Archmodels Vol.6 (Banyo Urun-Dolap-Musluk-Aks) PDFDocumento5 pagineArchmodels Vol.6 (Banyo Urun-Dolap-Musluk-Aks) PDFgene2693Nessuna valutazione finora
- Label Format AuditDocumento4 pagineLabel Format Auditgene2693Nessuna valutazione finora
- Philippine Regulation On Sanitation and Waste Water Systems by Bonifacio MagtibayDocumento193 paginePhilippine Regulation On Sanitation and Waste Water Systems by Bonifacio MagtibayRenee Rose GregorioNessuna valutazione finora
- Turb Mod NotesDocumento32 pagineTurb Mod NotessamandondonNessuna valutazione finora
- VVP Engg. CollegeDocumento32 pagineVVP Engg. Collegechotaimanav17Nessuna valutazione finora
- 14 BibiliographyDocumento22 pagine14 BibiliographyvaibhavNessuna valutazione finora
- Houses WorksheetDocumento3 pagineHouses WorksheetYeferzon Clavijo GilNessuna valutazione finora
- Project Management Pro: Powerpoint SlidesDocumento350 pagineProject Management Pro: Powerpoint SlidesJosephNessuna valutazione finora
- Interpretation of Statutes 2023 Question PaperDocumento4 pagineInterpretation of Statutes 2023 Question PaperNisha BhartiNessuna valutazione finora
- Independent Distributor Price List: DXN Bolivia S.R.LDocumento1 paginaIndependent Distributor Price List: DXN Bolivia S.R.LAdalid Llusco QuispeNessuna valutazione finora
- General Mathematics-FINALDocumento187 pagineGeneral Mathematics-FINALDummy AccountNessuna valutazione finora
- Ad&d - Poison Costs & Poison CraftDocumento4 pagineAd&d - Poison Costs & Poison Craftweb moriccaNessuna valutazione finora
- Gardens Illustrated FernandoDocumento4 pagineGardens Illustrated FernandoMariaNessuna valutazione finora
- B B B B: RRRR RRRRDocumento24 pagineB B B B: RRRR RRRRAnonymous TeF0kYNessuna valutazione finora
- AgrippaDocumento4 pagineAgrippaFloorkitNessuna valutazione finora
- German Employment Visa Application: What Is A German Work Visa and Do I Need One?Documento4 pagineGerman Employment Visa Application: What Is A German Work Visa and Do I Need One?FarbodNessuna valutazione finora
- CTY1 Assessments Unit 6 Review Test 1Documento5 pagineCTY1 Assessments Unit 6 Review Test 1'Shanned Gonzalez Manzu'Nessuna valutazione finora
- English Holiday TaskDocumento2 pagineEnglish Holiday Taskchandan2159Nessuna valutazione finora
- Robbins FOM10ge C05Documento35 pagineRobbins FOM10ge C05Ahmed Mostafa ElmowafyNessuna valutazione finora
- Pau Inglés-7Documento2 paginePau Inglés-7AlfodNessuna valutazione finora
- B. Complete The Following Exercise With or Forms of The Indicated VerbsDocumento4 pagineB. Complete The Following Exercise With or Forms of The Indicated VerbsLelyLealGonzalezNessuna valutazione finora
- VC++ Splitter Windows & DLLDocumento41 pagineVC++ Splitter Windows & DLLsbalajisathyaNessuna valutazione finora