Potrebbero piacerti anche
- How To Report A CT - Brain StudyDocumento17 pagineHow To Report A CT - Brain StudyJoanNessuna valutazione finora
- How To Report A CT - Brain StudyDocumento18 pagineHow To Report A CT - Brain StudyDrbaddireddy RayuduNessuna valutazione finora
- Basic CTDocumento71 pagineBasic CTRapid Medicine100% (2)
- Approach To Head CTDocumento31 pagineApproach To Head CTElisabeth F. Ojha100% (2)
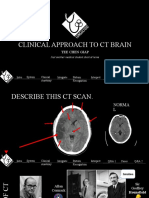
- Clinical Approach To CT BrainDocumento34 pagineClinical Approach To CT BrainXiaoThoong LohNessuna valutazione finora
- Community-Acquired Pneumonia: Strategies for ManagementDa EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresValutazione: 4.5 su 5 stelle4.5/5 (2)
- Brain CTDocumento83 pagineBrain CTArvind Jha100% (2)
- Hemoptysis - Case Presentation and DiscussionDocumento52 pagineHemoptysis - Case Presentation and DiscussionPGHC100% (1)
- Diffuse Parenchymal Lung DiseaseDocumento36 pagineDiffuse Parenchymal Lung DiseaseVeerapong Vattanavanit100% (1)
- Stroke: Intracranial Abnormalities With Hetal Verma, MDDocumento30 pagineStroke: Intracranial Abnormalities With Hetal Verma, MDRawabi rawabi1997Nessuna valutazione finora
- CSA Courses Cases Migraine PDFDocumento5 pagineCSA Courses Cases Migraine PDFSalah ElbadawyNessuna valutazione finora
- Psy MnemonicDocumento11 paginePsy MnemonicAmirul Hafiz100% (1)
- Normal Head CT AnatomyDocumento59 pagineNormal Head CT AnatomyDea Ritung100% (1)
- Interventional Neuroradiology A Complete Guide - 2020 EditionDa EverandInterventional Neuroradiology A Complete Guide - 2020 EditionNessuna valutazione finora
- Finals Neurology OSCEDocumento100 pagineFinals Neurology OSCERobin Abraham-BalisiNessuna valutazione finora
- Neurology PDFDocumento60 pagineNeurology PDFCahaya Al-HazeenillahNessuna valutazione finora
- Simple Note On Medical ApproachDocumento7 pagineSimple Note On Medical ApproachSyaidatul NadwaNessuna valutazione finora
- HemiplegiaDocumento30 pagineHemiplegiasarguss14100% (1)
- NeurologyDocumento118 pagineNeurologykep1313Nessuna valutazione finora
- How To Read A Head CT ScanDocumento60 pagineHow To Read A Head CT ScanPompomNessuna valutazione finora
- NeuroradiologyDocumento11 pagineNeuroradiologysarguss14100% (2)
- Clinical ExDocumento123 pagineClinical ExDeepti ChaharNessuna valutazione finora
- Brain ImagingDocumento56 pagineBrain ImagingAnant PachisiaNessuna valutazione finora
- Coma and Brain DeathDocumento21 pagineComa and Brain DeathDrGasnasNessuna valutazione finora
- CardiologyDocumento6 pagineCardiologyFrancis FransNessuna valutazione finora
- Common Histories and Red Flags Presentation Noninteractive VersionDocumento21 pagineCommon Histories and Red Flags Presentation Noninteractive VersionesmarNessuna valutazione finora
- Advice To Medical Students Studying Neurology - Docx - 4673Documento9 pagineAdvice To Medical Students Studying Neurology - Docx - 4673Anonymous vnv6QFNessuna valutazione finora
- PRO 2012 Short Case (Surgical) CompilationDocumento24 paginePRO 2012 Short Case (Surgical) CompilationvijayaNessuna valutazione finora
- Dental:: 2. OPG - Dentigerous CystDocumento56 pagineDental:: 2. OPG - Dentigerous CystVijay RanaNessuna valutazione finora
- Medicine Long CaseDocumento26 pagineMedicine Long Casewhee182Nessuna valutazione finora
- MBBS2014 SurgeryCaseAnalysisDocumento194 pagineMBBS2014 SurgeryCaseAnalysisDaniel LimNessuna valutazione finora
- Stroke Syndromes and Localization 2007Documento56 pagineStroke Syndromes and Localization 2007SaintPaul Univ100% (1)
- Lesion Localization in NeurologyDocumento34 pagineLesion Localization in NeurologyValeria Leon AbadNessuna valutazione finora
- Physiology System Specific Physiology (399Qs)Documento170 paginePhysiology System Specific Physiology (399Qs)rajvikram87Nessuna valutazione finora
- Journal Club Handbook: Sarah Massey Knowledge & Library Services Manager Illingworth LibraryDocumento20 pagineJournal Club Handbook: Sarah Massey Knowledge & Library Services Manager Illingworth Librarygehanath100% (2)
- Basic Approch To CT BrainDocumento62 pagineBasic Approch To CT BrainS B SayedNessuna valutazione finora
- Pre-Exam Preparation For Medicine (January 1, 2014) - (935152549X)Documento314 paginePre-Exam Preparation For Medicine (January 1, 2014) - (935152549X)RinkalNessuna valutazione finora
- 16 Stroke SyndromesDocumento32 pagine16 Stroke SyndromesRos Potter100% (2)
- Guidelines For OSCEsDocumento26 pagineGuidelines For OSCEsfrancieudo1Nessuna valutazione finora
- Approach To Neurological DiseaseDocumento68 pagineApproach To Neurological DiseaseNEuRoLoGisT CoFFeeCuPNessuna valutazione finora
- Neurology - Headache NotesDocumento3 pagineNeurology - Headache NotessarahNessuna valutazione finora
- Cns ExaminationDocumento17 pagineCns ExaminationJuana Maria Garcia Espinoza100% (1)
- Shivaani (Internal Medicine CWU)Documento12 pagineShivaani (Internal Medicine CWU)S.M. Manogaran Shivaani AP S.M. ManogaranNessuna valutazione finora
- O&g Osce BookletDocumento3 pagineO&g Osce BookletJohn TangNessuna valutazione finora
- Almostadoctor - co.uk-OSCE ChecklistDocumento10 pagineAlmostadoctor - co.uk-OSCE ChecklistJonathan YoungNessuna valutazione finora
- SPMM Smart Revise Descriptive Psychopathology Paper A Syllabic Content 5.22 Mrcpsych NoteDocumento43 pagineSPMM Smart Revise Descriptive Psychopathology Paper A Syllabic Content 5.22 Mrcpsych NoteBakir JaberNessuna valutazione finora
- Ultrasound Measurement Cheat SheetDocumento1 paginaUltrasound Measurement Cheat SheetDr. MLKNessuna valutazione finora
- How To Read A Chest X RayDocumento11 pagineHow To Read A Chest X RayHilmia Fahma100% (2)
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocumento69 pagineValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNessuna valutazione finora
- OSCE Qs Internal MedicineDocumento29 pagineOSCE Qs Internal MedicineRancesh Famo0% (1)
- Cranial NervesDocumento65 pagineCranial NervesatefmaboodNessuna valutazione finora
- Cardiology 2012 MrcppassDocumento127 pagineCardiology 2012 MrcppassRaouf Ra'fat SolimanNessuna valutazione finora
- Brain CT Essentials: Alexander Mamourian, MDDocumento223 pagineBrain CT Essentials: Alexander Mamourian, MDCoding NinjaNessuna valutazione finora
- CT BasicsDocumento43 pagineCT BasicsRumana AliNessuna valutazione finora
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDocumento43 pagine2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateKadek Aditya Darma YogaNessuna valutazione finora
- Bedside Medicine Without Tears Chugh PDFDocumento454 pagineBedside Medicine Without Tears Chugh PDFAishwaray KohliNessuna valutazione finora
- Crime PaperDocumento15 pagineCrime Paperyukta ambasthaNessuna valutazione finora
- H-046-003758-00 Wash Solution FDADocumento4 pagineH-046-003758-00 Wash Solution FDABagus KrisdianNessuna valutazione finora
- Specific Groups EssayDocumento1 paginaSpecific Groups Essaysunilvajshi2873Nessuna valutazione finora
- The 6 Nutrients WorksheetsDocumento4 pagineThe 6 Nutrients WorksheetschillNessuna valutazione finora
- Nafasi Za Kazi UdomDocumento25 pagineNafasi Za Kazi UdomSwalau OmaryNessuna valutazione finora
- Challenges Faced by Roma Women in EuropeDocumento29 pagineChallenges Faced by Roma Women in EuropeaurimiaNessuna valutazione finora
- Kerry Functional Health Benefits For Every GenerationDocumento18 pagineKerry Functional Health Benefits For Every GenerationNet SupraluckNessuna valutazione finora
- Argument EssayDocumento6 pagineArgument Essayapi-509629455Nessuna valutazione finora
- Digital Workflow For CAD-CAM Custom Abutments of Immediate Implants Based On Natural Emergence Profile of The Tooth To Be ExtractedDocumento23 pagineDigital Workflow For CAD-CAM Custom Abutments of Immediate Implants Based On Natural Emergence Profile of The Tooth To Be ExtractedRAEDNessuna valutazione finora
- Health Belief ModelDocumento12 pagineHealth Belief Modelmariatul fithriasariNessuna valutazione finora
- Theories of Personality: Rollo Reese MayDocumento4 pagineTheories of Personality: Rollo Reese MayShammah PradesNessuna valutazione finora
- MRCP BCC 2Documento5 pagineMRCP BCC 2zhichee91Nessuna valutazione finora
- Psychological TestingDocumento149 paginePsychological Testingxiejie22590Nessuna valutazione finora
- CBT QuestionsDocumento3 pagineCBT QuestionsdenfanNessuna valutazione finora
- Caregiving 12 Module 1 4th QuarterDocumento23 pagineCaregiving 12 Module 1 4th QuarterBethuel AlquirozNessuna valutazione finora
- CEA Regulations-2011 - PPT - 07 JUN 2016Documento47 pagineCEA Regulations-2011 - PPT - 07 JUN 2016Rajeev Sharma100% (1)
- Gender Support Plan PDFDocumento4 pagineGender Support Plan PDFGender SpectrumNessuna valutazione finora
- 12.1 Guided ReadingDocumento2 pagine12.1 Guided ReadingGrant HasletonNessuna valutazione finora
- Analysis of Acceptance of E-Health Application by Users in Primary Healthcare Center in Surabaya CityDocumento13 pagineAnalysis of Acceptance of E-Health Application by Users in Primary Healthcare Center in Surabaya Citynurul ismatullahNessuna valutazione finora
- Nurse To Patient RatioDocumento7 pagineNurse To Patient RatioNeng IkaNessuna valutazione finora
- Disruptive Mood Dysregulation DisorderDocumento13 pagineDisruptive Mood Dysregulation DisorderNyoman SuryaNessuna valutazione finora
- LESSON 3: Exercise Variables and PrinciplesDocumento31 pagineLESSON 3: Exercise Variables and PrinciplesCapulong Kimberly100% (1)
- Fetal DevelopmentDocumento15 pagineFetal DevelopmentOmar HammadNessuna valutazione finora
- Q2 Phil. Politics & Governance 12 Module 2Documento17 pagineQ2 Phil. Politics & Governance 12 Module 2Hannah Mae ArsenioNessuna valutazione finora
- OSSSC Diploma in Pharmacy..Documento8 pagineOSSSC Diploma in Pharmacy..RAJANI SathuaNessuna valutazione finora
- CDC Misinformation EmailsDocumento76 pagineCDC Misinformation EmailsZerohedge Janitor100% (2)
- Wcms - 618575 31 70 28 34Documento7 pagineWcms - 618575 31 70 28 34alin grecuNessuna valutazione finora
- Hormones Informed-Consent-Guidelines DIGITALDocumento50 pagineHormones Informed-Consent-Guidelines DIGITALcarmenrossittoNessuna valutazione finora
- Professional Growth Plan New VersionDocumento4 pagineProfessional Growth Plan New VersionAlechia Fludd77% (13)
- 03 MSDS BentoniteDocumento5 pagine03 MSDS BentoniteFurqan SiddiquiNessuna valutazione finora