Potrebbero piacerti anche
- Practical Trends in Anesthesia and Intensive Care 2018Da EverandPractical Trends in Anesthesia and Intensive Care 2018Nessuna valutazione finora
- 508 - 7 CardiologyDocumento9 pagine508 - 7 CardiologymlinaballerinaNessuna valutazione finora
- Compresor Intermitente TVPDocumento9 pagineCompresor Intermitente TVPgiseladelarosa2006Nessuna valutazione finora
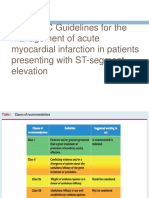
- 2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment ElevationDocumento62 pagine2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment ElevationNurcahyaKuswardhanaNessuna valutazione finora
- Pi Is 0007091217540015Documento10 paginePi Is 0007091217540015Yoga WibowoNessuna valutazione finora
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocumento9 pagineReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNessuna valutazione finora
- 296 Neck of Femur Fracture Peri-Operative ManagementDocumento8 pagine296 Neck of Femur Fracture Peri-Operative ManagementNilam dwinilamsariNessuna valutazione finora
- Endovascular Stentgraft Placement in Aortic Dissection A MetaanalysisDocumento10 pagineEndovascular Stentgraft Placement in Aortic Dissection A MetaanalysisCiubuc AndrianNessuna valutazione finora
- Evidence-Based Perioperative Medicine (EBPOM) : A Summary of The 8th EBPOM Conference 2009Documento6 pagineEvidence-Based Perioperative Medicine (EBPOM) : A Summary of The 8th EBPOM Conference 2009ashut1Nessuna valutazione finora
- Anaesthesia 1Documento9 pagineAnaesthesia 1Sreekanth JangamNessuna valutazione finora
- Trauma Assessment Initial Trauma AssessmentDocumento6 pagineTrauma Assessment Initial Trauma Assessmentrika100% (1)
- Prehospital Thrombolysis: It S All About Time: February 2012Documento23 paginePrehospital Thrombolysis: It S All About Time: February 2012deo rizkyNessuna valutazione finora
- Surgical ComDocumento13 pagineSurgical ComVanitha VeeNessuna valutazione finora
- 1 s2.0 S0007091217542075 MainDocumento11 pagine1 s2.0 S0007091217542075 Maineny_sumaini65Nessuna valutazione finora
- MICS RWG Protocol 1Documento9 pagineMICS RWG Protocol 1jezreel terreNessuna valutazione finora
- TX Iskemik StrokeDocumento17 pagineTX Iskemik StrokeNailis Sa'adahNessuna valutazione finora
- Perioperative Anesthesia Anagement OnDocumento30 paginePerioperative Anesthesia Anagement OnryandikaNessuna valutazione finora
- Bernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?Documento26 pagineBernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?om mkNessuna valutazione finora
- Fernandes 2016Documento7 pagineFernandes 2016Hazem HashemNessuna valutazione finora
- Early Use of TIPS in Cirrhosis and Variceal BleedingDocumento10 pagineEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNessuna valutazione finora
- Managementul Acut Al TVC La Cei in Tratament Cu AntiagregantDocumento21 pagineManagementul Acut Al TVC La Cei in Tratament Cu AntiagregantDrHellenNessuna valutazione finora
- Outcomes of Primary Percutaneous Coronary Intervention in Acute Myocardial Infarction at Tehran Heart CenterDocumento6 pagineOutcomes of Primary Percutaneous Coronary Intervention in Acute Myocardial Infarction at Tehran Heart CenterHamiNessuna valutazione finora
- Immediate and Long Term Outcomes Following Orthopedic Procedures in - 2019 - BLDocumento4 pagineImmediate and Long Term Outcomes Following Orthopedic Procedures in - 2019 - BLMichael John AguilarNessuna valutazione finora
- Current Concepts in Management of Polytrauma PatientDocumento12 pagineCurrent Concepts in Management of Polytrauma PatientSuresh KumarNessuna valutazione finora
- s12872 019 1096 1Documento9 pagines12872 019 1096 1sarahNessuna valutazione finora
- A Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalDocumento4 pagineA Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalHaziq AnuarNessuna valutazione finora
- Percutaneous Transluminal Coronary Angioplasty (PTCA) and Stenting - Study of 100 CasesDocumento7 paginePercutaneous Transluminal Coronary Angioplasty (PTCA) and Stenting - Study of 100 CasesLuqy Luqman EffendyNessuna valutazione finora
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDocumento6 pagineTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142Nessuna valutazione finora
- Bmri2016 3741426Documento7 pagineBmri2016 3741426MandaNessuna valutazione finora
- New England Journal Medicine: The ofDocumento13 pagineNew England Journal Medicine: The ofAlexei Ricse JiménezNessuna valutazione finora
- Outcome Predictors of Acute Stroke Patients in Need of Intensive Care TreatmentDocumento8 pagineOutcome Predictors of Acute Stroke Patients in Need of Intensive Care TreatmentAstrid CarolineNessuna valutazione finora
- Impact of Postoperative Morbidity On Long-Term Survival After OesophagectomyDocumento10 pagineImpact of Postoperative Morbidity On Long-Term Survival After OesophagectomyPutri PadmosuwarnoNessuna valutazione finora
- The Impact of Closed Incision Negative Pressure Therapy On Prevention of Median Sternotomy Infection For High Risk Cases: A Single Centre Retrospective StudyDocumento9 pagineThe Impact of Closed Incision Negative Pressure Therapy On Prevention of Median Sternotomy Infection For High Risk Cases: A Single Centre Retrospective StudyfabiolaNessuna valutazione finora
- STITCH Protocol 2011Documento9 pagineSTITCH Protocol 2011Crhistian GarcíaNessuna valutazione finora
- PolipillDocumento10 paginePolipillSMIBA MedicinaNessuna valutazione finora
- Aep 373Documento7 pagineAep 373Salsabila FitriaNessuna valutazione finora
- Preliminary Experience With Cangrelor For Endovascular Treatment ofDocumento9 paginePreliminary Experience With Cangrelor For Endovascular Treatment ofPedro VillamorNessuna valutazione finora
- J Thromb Thrombolysis 2020 Sep 14 Smith DDocumento8 pagineJ Thromb Thrombolysis 2020 Sep 14 Smith DFernando SousaNessuna valutazione finora
- Cancers 14 03845Documento15 pagineCancers 14 03845regigaby02Nessuna valutazione finora
- Trauma Assessment Initial Trauma AssessmentDocumento5 pagineTrauma Assessment Initial Trauma AssessmentzulfahNessuna valutazione finora
- Cannon Jeremy Multicenter Studies MaterialsDocumento14 pagineCannon Jeremy Multicenter Studies MaterialsSamer Al-BothaigiNessuna valutazione finora
- Clinical StudyDocumento7 pagineClinical StudyAldo AtjehNessuna valutazione finora
- Problems and Solutions in The Implementation of A Transcatheter Aortic Valve Implantation ProgramDocumento6 pagineProblems and Solutions in The Implementation of A Transcatheter Aortic Valve Implantation ProgramJc GaldosNessuna valutazione finora
- Goyal Et Al-2015-Annals of NeurologyDocumento7 pagineGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNessuna valutazione finora
- Jurnal THTDocumento3 pagineJurnal THTValentina AdindaNessuna valutazione finora
- JofIMAB2013vol19b2p282 285 PDFDocumento4 pagineJofIMAB2013vol19b2p282 285 PDFAlung Padang SiraitNessuna valutazione finora
- European Guidelines On Perioperative Venous.11Documento5 pagineEuropean Guidelines On Perioperative Venous.11ionut.andruscaNessuna valutazione finora
- Fibrinolysis or Primary PCI in STDocumento6 pagineFibrinolysis or Primary PCI in STFachry MuhammadNessuna valutazione finora
- Clinical Trials and Regulatory Science in CardiologyDocumento6 pagineClinical Trials and Regulatory Science in Cardiologydianaerlita97Nessuna valutazione finora
- Prehospital Stroke Care: New Prospects For Treatment and Clinical ResearchDocumento8 paginePrehospital Stroke Care: New Prospects For Treatment and Clinical ResearchmiriamneuroNessuna valutazione finora
- Imaging Predictors of Procedural and Clinical OutcDocumento13 pagineImaging Predictors of Procedural and Clinical OutcYusuf BrilliantNessuna valutazione finora
- Mobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournDocumento7 pagineMobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournStefan LaurentiuNessuna valutazione finora
- Summary 2014 Esc GuidelinesDocumento13 pagineSummary 2014 Esc GuidelinesNick StamatiadisNessuna valutazione finora
- Diagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockDocumento7 pagineDiagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockPaul CalbureanNessuna valutazione finora
- Biomedicines 11 00979Documento10 pagineBiomedicines 11 00979akinaNessuna valutazione finora
- Efficacy and Safety o A Dedicated LAAO Protocol 2022Documento3 pagineEfficacy and Safety o A Dedicated LAAO Protocol 2022吳醫師Nessuna valutazione finora
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocumento6 paginePercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNessuna valutazione finora
- Safety and Efficacy of Tirofiban Combined With Endovascular Treatment in Acute Ischaemic StrokeDocumento6 pagineSafety and Efficacy of Tirofiban Combined With Endovascular Treatment in Acute Ischaemic StrokeJorge Luis Plasencia CubaNessuna valutazione finora
- Acute Ischaemic StrokeDocumento40 pagineAcute Ischaemic StrokeDana Crusoveanu100% (1)
- Guias ASRA 2010 Anestesia Regional en Paciente AnticoaguladoDocumento38 pagineGuias ASRA 2010 Anestesia Regional en Paciente AnticoaguladoJonathan Tipon Galvis100% (1)
- Modified Jailed Balloon Technique For Coronary Artery Bifurcation LesionsDocumento3 pagineModified Jailed Balloon Technique For Coronary Artery Bifurcation LesionsMonica TrifitrianaNessuna valutazione finora
- Chen 2016 NewDocumento9 pagineChen 2016 NewMonica TrifitrianaNessuna valutazione finora
- Chen 2016Documento9 pagineChen 2016Monica TrifitrianaNessuna valutazione finora
- Dai 2015Documento7 pagineDai 2015Monica TrifitrianaNessuna valutazione finora
- Drożdż 2019Documento7 pagineDrożdż 2019Monica TrifitrianaNessuna valutazione finora
- Permanent Pacing in Patients Without Upper Limb Access PDFDocumento4 paginePermanent Pacing in Patients Without Upper Limb Access PDFMonica TrifitrianaNessuna valutazione finora
- Cardiac Pacemaker UtamaDocumento23 pagineCardiac Pacemaker UtamaMonica Trifitriana100% (1)
- Paglia Cardiac Pacemaker Utama PDFDocumento23 paginePaglia Cardiac Pacemaker Utama PDFMonica TrifitrianaNessuna valutazione finora
- Pacemaker Trough Jugular Internal VeinDocumento3 paginePacemaker Trough Jugular Internal VeinMonica TrifitrianaNessuna valutazione finora
- Faktor Umur Terhadap Oklusi Dan Trombosis PDFDocumento19 pagineFaktor Umur Terhadap Oklusi Dan Trombosis PDFMonica TrifitrianaNessuna valutazione finora
- 26 PDFDocumento13 pagine26 PDFMonica TrifitrianaNessuna valutazione finora
- Permanent Pacemaker TechniqueDocumento7 paginePermanent Pacemaker TechniqueMonica TrifitrianaNessuna valutazione finora
- Seow Permanent Pacing in Patients Without Upper Limb Access PDFDocumento4 pagineSeow Permanent Pacing in Patients Without Upper Limb Access PDFMonica TrifitrianaNessuna valutazione finora
- Predictors of OclusionDocumento6 paginePredictors of OclusionMonica TrifitrianaNessuna valutazione finora
- PMCC PF Support PermanentPacemakersDocumento10 paginePMCC PF Support PermanentPacemakersMonica TrifitrianaNessuna valutazione finora
- Vein Management For Cardiac Device ImplantationDocumento11 pagineVein Management For Cardiac Device ImplantationMonica TrifitrianaNessuna valutazione finora
- Seow Permanent Pacing in Patients Without Upper Limb Access PDFDocumento4 pagineSeow Permanent Pacing in Patients Without Upper Limb Access PDFMonica TrifitrianaNessuna valutazione finora
- Vein Management For Cardiac Device Implantation PDFDocumento11 pagineVein Management For Cardiac Device Implantation PDFMonica TrifitrianaNessuna valutazione finora
- 23 PDFDocumento5 pagine23 PDFMonica TrifitrianaNessuna valutazione finora
- Kotsakou Pacemaker Insertion PDFDocumento8 pagineKotsakou Pacemaker Insertion PDFMonica TrifitrianaNessuna valutazione finora
- Risk of Motratility Post PPMDocumento6 pagineRisk of Motratility Post PPMMonica TrifitrianaNessuna valutazione finora
- 26 PDFDocumento13 pagine26 PDFMonica TrifitrianaNessuna valutazione finora
- Jurnal Ballon Stent Kissing For Interventional Bifucuration Vs Jailed Wire PDFDocumento6 pagineJurnal Ballon Stent Kissing For Interventional Bifucuration Vs Jailed Wire PDFMonica TrifitrianaNessuna valutazione finora
- Classification of Coronary Artery Bifurcation Lesions and TreatmentDocumento9 pagineClassification of Coronary Artery Bifurcation Lesions and TreatmentMonica TrifitrianaNessuna valutazione finora
- 25 PDFDocumento16 pagine25 PDFMonica TrifitrianaNessuna valutazione finora
- 9746 A Systematic Literature Review of Three Stenting Strategies For Bifurcation Lesions in Coronary Artery DiseaseDocumento11 pagine9746 A Systematic Literature Review of Three Stenting Strategies For Bifurcation Lesions in Coronary Artery DiseaseMonica TrifitrianaNessuna valutazione finora
- Reabilitare Dupa AvcDocumento91 pagineReabilitare Dupa AvcDiana StancaNessuna valutazione finora
- Ashiq Tutorials 2008Documento23 pagineAshiq Tutorials 2008Sk ChaudhryNessuna valutazione finora
- Acog Practice Bulletin: Thromboembolism in PregnancyDocumento17 pagineAcog Practice Bulletin: Thromboembolism in PregnancytriNessuna valutazione finora
- Leg EdemaDocumento13 pagineLeg Edemacamila perillaNessuna valutazione finora
- COVID 19 Is A Systemic Vascular HemopathyDocumento34 pagineCOVID 19 Is A Systemic Vascular HemopathyYuri YogyaNessuna valutazione finora
- D Dimer Test in VTEDocumento35 pagineD Dimer Test in VTEscribmedNessuna valutazione finora
- Enoxaparin FDADocumento40 pagineEnoxaparin FDAImam Nur Alif Khusnudin100% (2)
- New Patient Needing Continuous Renal Replacement Therapy (CRRT)Documento9 pagineNew Patient Needing Continuous Renal Replacement Therapy (CRRT)sergey_1972Nessuna valutazione finora
- AC After StrokeDocumento6 pagineAC After StrokeDileepa chathurangaNessuna valutazione finora
- Diane 35 PM en PDFDocumento44 pagineDiane 35 PM en PDFAhmad MuhlisinNessuna valutazione finora
- Oxford McqsDocumento15 pagineOxford McqsaliaaNessuna valutazione finora
- Summary of Product CharacteristicsDocumento24 pagineSummary of Product Characteristicsddandan_2Nessuna valutazione finora
- Tranexamic Acid A Narrative Review For The Emergency Medicine Clinician Am J Emerg Med 2022Documento12 pagineTranexamic Acid A Narrative Review For The Emergency Medicine Clinician Am J Emerg Med 2022Dra. Lizbeth Lira HerreraNessuna valutazione finora
- Anticoagulants and Antiplatelet AgentsDocumento4 pagineAnticoagulants and Antiplatelet AgentsMark Russel Sean LealNessuna valutazione finora
- Toxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDDocumento8 pagineToxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDGoran TomićNessuna valutazione finora
- Xodo Document - Periprocedural - Anticoagulation - GuidelineDocumento16 pagineXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xNessuna valutazione finora
- DVTDocumento4 pagineDVTMàŗwā TāhāNessuna valutazione finora
- Leunase and TrombolismDocumento12 pagineLeunase and TrombolismSanta UlinaNessuna valutazione finora
- Premarin Drug StudyDocumento8 paginePremarin Drug StudyjanNessuna valutazione finora
- Summary Chart of U.S. Medical Eligibility Criteria For Contraceptive UseDocumento2 pagineSummary Chart of U.S. Medical Eligibility Criteria For Contraceptive UseBlessy AbrahamNessuna valutazione finora
- DVT ProphylaxisDocumento30 pagineDVT ProphylaxisedhsnzktNessuna valutazione finora
- Passmrcog Patho, Embryo 2016Documento171 paginePassmrcog Patho, Embryo 2016Mona HelouNessuna valutazione finora
- ClexaneDocumento19 pagineClexaneahmadNessuna valutazione finora
- Drug Monograph ExampleDocumento6 pagineDrug Monograph ExampleAaltiyaNessuna valutazione finora
- STD Heparin Protocol MethodistDocumento1 paginaSTD Heparin Protocol Methodistd40sithuiNessuna valutazione finora
- CH3 Patho D&R AgamDocumento30 pagineCH3 Patho D&R AgamS Balagopal SivaprakasamNessuna valutazione finora
- Surgery MCQ-1Documento35 pagineSurgery MCQ-1Fan Eli100% (15)
- Noxarin Brosur-MinDocumento4 pagineNoxarin Brosur-MinAndy RahadianNessuna valutazione finora
- Gynera: Coated TabletsDocumento67 pagineGynera: Coated TabletsOdeke VascoNessuna valutazione finora
- UPDATE MENEJEMEN DVTDocumento9 pagineUPDATE MENEJEMEN DVTSupandy HasanNessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Da EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Valutazione: 5 su 5 stelle5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDa EverandGut: the new and revised Sunday Times bestsellerValutazione: 4 su 5 stelle4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDa EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningValutazione: 4 su 5 stelle4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Da EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Valutazione: 4 su 5 stelle4/5 (378)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (58)