Potrebbero piacerti anche
- Advances in The Treatment of RootDocumento21 pagineAdvances in The Treatment of RootRamona MateiNessuna valutazione finora
- Allergic Reactions in EndodonticDocumento8 pagineAllergic Reactions in EndodonticDr.O.R.GANESAMURTHINessuna valutazione finora
- Aetiology and Rates of Treatment of Traumatic PDFDocumento6 pagineAetiology and Rates of Treatment of Traumatic PDFRamona MateiNessuna valutazione finora
- Aetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailDocumento10 pagineAetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailFlorin IonescuNessuna valutazione finora
- An Alternative Method For Splinting of PDFDocumento5 pagineAn Alternative Method For Splinting of PDFRamona MateiNessuna valutazione finora
- An in Vitro Study of The PH of Three CalciumDocumento5 pagineAn in Vitro Study of The PH of Three CalciumRamona MateiNessuna valutazione finora
- 2005 BR Dent J - Anterior Dental Aesthetics - Dental PerspectiveDocumento7 pagine2005 BR Dent J - Anterior Dental Aesthetics - Dental PerspectiveLucero Salvatierra BrionesNessuna valutazione finora
- An in Vitro Evaluation of The Antimicrobial Efficacy of Irrigants On Biofilms of Root Canal Isolates PDFDocumento8 pagineAn in Vitro Evaluation of The Antimicrobial Efficacy of Irrigants On Biofilms of Root Canal Isolates PDFDiverse AnunturiNessuna valutazione finora
- Anatomia Del Piso de La Cámara Pulpar KRASNER JOE 2004 PDFDocumento12 pagineAnatomia Del Piso de La Cámara Pulpar KRASNER JOE 2004 PDFMatthew Lama CordovaNessuna valutazione finora
- Analysis of Complications Following Alveolar Distraction OsteogenesisDocumento6 pagineAnalysis of Complications Following Alveolar Distraction OsteogenesisRamona MateiNessuna valutazione finora
- An Oral Health Promotion Program ForDocumento5 pagineAn Oral Health Promotion Program ForRamona MateiNessuna valutazione finora
- Analysis of 154 Cases of Teeth With CracksDocumento6 pagineAnalysis of 154 Cases of Teeth With CracksRamona MateiNessuna valutazione finora
- Anterior Palatal Mouthguard Margin LocationDocumento6 pagineAnterior Palatal Mouthguard Margin LocationRamona MateiNessuna valutazione finora
- Analysis of Pulpal Reactions To Restorative Procedures, Materials, Pulp Capping, and Future TherapiesDocumento12 pagineAnalysis of Pulpal Reactions To Restorative Procedures, Materials, Pulp Capping, and Future TherapiesAmr EldokNessuna valutazione finora
- 4812521a PDFDocumento8 pagine4812521a PDFbkprosthoNessuna valutazione finora
- Apical Anatomy in Mesial and Mesiobuccal RootsDocumento5 pagineApical Anatomy in Mesial and Mesiobuccal RootsFlorin IonescuNessuna valutazione finora
- Aesthetid 2Documento7 pagineAesthetid 2hmsatNessuna valutazione finora
- Aesthetics 5Documento8 pagineAesthetics 5drsmritiNessuna valutazione finora
- Apical Limit PDFDocumento16 pagineApical Limit PDFDiverse AnunturiNessuna valutazione finora
- Antibiotic Prophylaxis PDFDocumento14 pagineAntibiotic Prophylaxis PDFDiverse AnunturiNessuna valutazione finora
- 1.historical PerspectiveDocumento6 pagine1.historical PerspectiveJyothsna S ReddyNessuna valutazione finora
- Antibacterial Effect of Ca (OH) 2 - Systematic Review IEJ 2006Documento9 pagineAntibacterial Effect of Ca (OH) 2 - Systematic Review IEJ 2006Ramona MateiNessuna valutazione finora
- Antibiotic Coverage For Lip WoundDocumento1 paginaAntibiotic Coverage For Lip WoundRamona MateiNessuna valutazione finora
- Apexification A ReviewDocumento8 pagineApexification A ReviewMohammed Ali Alazrak100% (1)
- Apoptosis in Epithelial Cells of Apical Radicular Cysts PDFDocumento5 pagineApoptosis in Epithelial Cells of Apical Radicular Cysts PDFRamona MateiNessuna valutazione finora
- Apical Limit of Root Canal Instrumentation and Obturation, PDocumento10 pagineApical Limit of Root Canal Instrumentation and Obturation, PRamona MateiNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Jurnal Tara SyifaDocumento4 pagineJurnal Tara SyifaMuhammad Fauzan IhsanNessuna valutazione finora
- Roth VS MBT PDFDocumento4 pagineRoth VS MBT PDFJoshua Stalin0% (1)
- ACC Soft Tissue Development Around Pontic SiteDocumento5 pagineACC Soft Tissue Development Around Pontic SiteJayarti Rohmadani MarsaNessuna valutazione finora
- Non-Competitive Research Paper PresentationsDocumento17 pagineNon-Competitive Research Paper PresentationsRinkle SardanaNessuna valutazione finora
- A Review On Toothbrushes and Tooth Brushing MethodsDocumento10 pagineA Review On Toothbrushes and Tooth Brushing MethodsinventionjournalsNessuna valutazione finora
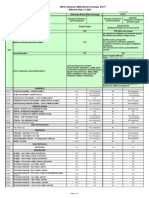
- MCS Classicare (MA) Dental Coverage SummaryDocumento4 pagineMCS Classicare (MA) Dental Coverage SummaryJessicaNessuna valutazione finora
- FMR With SplintDocumento5 pagineFMR With SplintDr Tarak ChavadaNessuna valutazione finora
- Long Face SyndromeDocumento144 pagineLong Face Syndromeavanthika krishnaraj100% (2)
- Radiographic features and treatment of periapical cystDocumento40 pagineRadiographic features and treatment of periapical cystLojin HaddadNessuna valutazione finora
- Prpposal Presentation Oct 2011 RevDocumento34 paginePrpposal Presentation Oct 2011 RevLeilawati SulaimanNessuna valutazione finora
- 2003 124 5 509 514 BeckerDocumento6 pagine2003 124 5 509 514 BeckerFourthMolar.comNessuna valutazione finora
- Tooth Erosion, Attrition, Abrasion & AbfractionDocumento8 pagineTooth Erosion, Attrition, Abrasion & AbfractionCharlie McdonnellNessuna valutazione finora
- Gingival EnlargementCORRECTEDDocumento7 pagineGingival EnlargementCORRECTEDLita DamafitraNessuna valutazione finora
- Articulators 141010163229 Conversion Gate01Documento80 pagineArticulators 141010163229 Conversion Gate01Kanmani AthiNessuna valutazione finora
- The Use of Stainless Steel Crowns: Position PaperDocumento5 pagineThe Use of Stainless Steel Crowns: Position PaperMax FerNessuna valutazione finora
- Dental Anatomy & Occlusion NOTESDocumento7 pagineDental Anatomy & Occlusion NOTESyosman1000100% (1)
- IPS E.max Lithium Disilicate Technical UpdateDocumento2 pagineIPS E.max Lithium Disilicate Technical UpdateIvoclar Vivadent100% (1)
- Fixed prosthodontics editors and smile factorsDocumento5 pagineFixed prosthodontics editors and smile factorsJOSICA058100% (2)
- Bio Dentalbio Dental ResedaDocumento2 pagineBio Dentalbio Dental ResedamybiodentalNessuna valutazione finora
- Pcrs Handbook For Dentists HSEDocumento58 paginePcrs Handbook For Dentists HSESimona BudauNessuna valutazione finora
- Lecture-What Is OcclusionDocumento38 pagineLecture-What Is OcclusionAla Yassin100% (2)
- 5th Topic C - Oral Care ChecklistDocumento4 pagine5th Topic C - Oral Care ChecklistKhylamarie VillalunaNessuna valutazione finora
- PeriodontitisDocumento41 paginePeriodontitisJonasNessuna valutazione finora
- Implant DentistryDocumento11 pagineImplant DentistryDentist ChandraShekarNessuna valutazione finora
- Case Report: PRR Using Cention N in Children's TeethDocumento7 pagineCase Report: PRR Using Cention N in Children's TeethArevamadeline AegesfiNessuna valutazione finora
- Association Between Molar-Incisor Hypomineralization and Enamel HypoplasiaDocumento5 pagineAssociation Between Molar-Incisor Hypomineralization and Enamel HypoplasiaJonnathan MolinaNessuna valutazione finora
- Guardian - Dental PPO Plan Summary 2022Documento4 pagineGuardian - Dental PPO Plan Summary 2022Jessi ChallagullaNessuna valutazione finora
- Revascularization-Associated Intracanal Calcification: A Case Report With An 8-Year ReviewDocumento4 pagineRevascularization-Associated Intracanal Calcification: A Case Report With An 8-Year ReviewIvan PolancoNessuna valutazione finora
- Rest N Minor ConnectorDocumento74 pagineRest N Minor ConnectorNaveen ThakurNessuna valutazione finora
- Paper CanalDocumento23 paginePaper CanalCarlos Pizarro CórdovaNessuna valutazione finora