Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma in China Shen Et Al
Caricato da
Beverly TranCopyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma in China Shen Et Al
Caricato da
Beverly TranCopyright:
Formati disponibili
Research
JAMA | Preliminary Communication
Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma
Chenguang Shen, PhD; Zhaoqin Wang, PhD; Fang Zhao, PhD; Yang Yang, MD; Jinxiu Li, MD; Jing Yuan, MD; Fuxiang Wang, MD;
Delin Li, PhD; Minghui Yang, PhD; Li Xing, MM; Jinli Wei, MM; Haixia Xiao, PhD; Yan Yang, MM; Jiuxin Qu, MD; Ling Qing, MM;
Li Chen, MD; Zhixiang Xu, MM; Ling Peng, MM; Yanjie Li, MM; Haixia Zheng, MM; Feng Chen, MM; Kun Huang, MM; Yujing
Jiang, MM; Dongjing Liu, MD; Zheng Zhang, MD; Yingxia Liu, MD; Lei Liu, MD
Editorial
IMPORTANCE Coronavirus disease 2019 (COVID-19) is a pandemic with no specific Audio and Video and
therapeutic agents and substantial mortality. It is critical to find new treatments. Supplemental content
OBJECTIVE To determine whether convalescent plasma transfusion may be beneficial in the
treatment of critically ill patients with severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) infection.
DESIGN, SETTING, AND PARTICIPANTS Case series of 5 critically ill patients with
laboratory-confirmed COVID-19 and acute respiratory distress syndrome (ARDS) who met the
following criteria: severe pneumonia with rapid progression and continuously high viral load
despite antiviral treatment; PAO2/FIO2 <300; and mechanical ventilation. All 5 were treated
with convalescent plasma transfusion. The study was conducted at the infectious disease
department, Shenzhen Third People's Hospital in Shenzhen, China, from January 20, 2020,
to March 25, 2020; final date of follow-up was March 25, 2020. Clinical outcomes were
compared before and after convalescent plasma transfusion.
EXPOSURES Patients received transfusion with convalescent plasma with a SARS-CoV-2–
specific antibody (IgG) binding titer greater than 1:1000 (end point dilution titer, by
enzyme-linked immunosorbent assay [ELISA]) and a neutralization titer greater than 40 (end
point dilution titer) that had been obtained from 5 patients who recovered from COVID-19.
Convalescent plasma was administered between 10 and 22 days after admission.
MAIN OUTCOMES AND MEASURES Changes of body temperature, Sequential Organ Failure
Assessment (SOFA) score (range 0-24, with higher scores indicating more severe illness),
PAO2/FIO2, viral load, serum antibody titer, routine blood biochemical index, ARDS, and
ventilatory and extracorporeal membrane oxygenation (ECMO) supports before and after
convalescent plasma transfusion.
RESULTS All 5 patients (age range, 36-65 years; 2 women) were receiving mechanical
ventilation at the time of treatment and all had received antiviral agents and
methylprednisolone. Following plasma transfusion, body temperature normalized within 3
days in 4 of 5 patients, the SOFA score decreased, and PAO2/FIO2 increased within 12 days
(range, 172-276 before and 284-366 after). Viral loads also decreased and became negative
within 12 days after the transfusion, and SARS-CoV-2–specific ELISA and neutralizing antibody
titers increased following the transfusion (range, 40-60 before and 80-320 on day 7). ARDS
resolved in 4 patients at 12 days after transfusion, and 3 patients were weaned from
mechanical ventilation within 2 weeks of treatment. Of the 5 patients, 3 have been
discharged from the hospital (length of stay: 53, 51, and 55 days), and 2 are in stable condition
at 37 days after transfusion.
CONCLUSIONS AND RELEVANCE In this preliminary uncontrolled case series of 5 critically ill
patients with COVID-19 and ARDS, administration of convalescent plasma containing Author Affiliations: Author
neutralizing antibody was followed by improvement in their clinical status. The limited sample affiliations are listed at the end of this
size and study design preclude a definitive statement about the potential effectiveness of this article.
treatment, and these observations require evaluation in clinical trials. Corresponding Authors: Yingxia
Liu, MD (yingxialiu@hotmail.com),
Zheng Zhang, MD (zhangzheng1975
@aliyun.com), and Lei Liu, MD
(liulei3322@aliyun.com), Shenzhen
Third People’s Hospital, Second
Hospital Affiliated to Southern
University of Science and Technology,
JAMA. doi:10.1001/jama.2020.4783 No. 29, Bulan Road, Longgang
Published online March 27, 2020. District, Shenzhen 518112, China.
(Reprinted) E1
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Research Preliminary Communication Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma
T
he epidemic of severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) originating in Wuhan, Key Points
China, has rapidly spread worldwide.1 As of March 24,
Question Could administration of convalescent plasma
2020, China had reported 81 767 cases with 3281 deaths, and transfusion be beneficial in the treatment of critically ill patients
the World Health Organization declared coronavirus disease with coronavirus disease 2019 (COVID-19)?
2019 (COVID-19) a pandemic. As of March 18, 2020, cases
Findings In this uncontrolled case series of 5 critically ill patients
were reported in approximately 195 countries.2
with COVID-19 and acute respiratory distress syndrome (ARDS),
No specific therapeutic agents or vaccines for COVID-19 are administration of convalescent plasma containing neutralizing
available.3 Several therapies, such as remdesivir and favipira- antibody was followed by an improvement in clinical status.
vir, are under investigation,3,4 but the antiviral efficacy of these
Meaning These preliminary findings raise the possibility that
drugs is not yet known. The use of convalescent plasma was
convalescent plasma transfusion may be helpful in the treatment
recommended as an empirical treatment during outbreaks of of critically ill patients with COVID-19 and ARDS, but this approach
Ebola virus in 2014, and a protocol for treatment of Middle East requires evaluation in randomized clinical trials.
respiratory syndrome coronavirus with convalescent plasma
was established in 2015.5 This approach with other viral infec-
tions such as SARS-CoV, H5N1 avian influenza, and H1N1 in- potential compatibility with the convalescent plasma donor, and
fluenza also suggested that transfusion of convalescent plasma each received 2 consecutive transfusions of 200 to 250 mL of
was effective.6-10 In previous reports, most of the patients re- ABO-compatible convalescent plasma (400 mL of convales-
ceived the convalescent plasma by single transfusion.9-11 In a cent plasma in total) on the same day it was obtained from the
study involving patients with pandemic influenza A(H1N1) 2009 donor. The patients received antiviral agents continuously un-
virus infection, treatment of severe infection with convales- til the SARS-CoV-2 viral loads became negative.
cent plasma (n = 20 patients) was associated with reduced re-
spiratory tract viral load, serum cytokine response, and Disease Severity Classification
mortality.10 In another study involving 80 patients with SARS, Patients with laboratory-confirmed COVID-19 infection who
administration of convalescent plasma was associated with a had any of the following were considered in critical condi-
higher rate of hospital bxdischarge at day 22 from symptom on- tion: (1) respiratory failure requiring mechanical ventilation,
set compared with patients who did not receive convalescent (2) shock, identified by the use of vasopressor therapy and el-
plasma.12 Accordingly, these findings raise the hypothesis that evated lactate levels (>2 mmol/L) despite adequate fluid re-
use of convalescent plasma transfusion could be beneficial in suscitation, or (3) failure of other organs requiring admission
patients infected with SARS-CoV-2. to the intensive care unit (ICU).
The purpose of this study was to describe the initial clini-
cal experience with convalescent plasma transfusion admin- Donors
istered to critically ill patients with COVID-19. The 5 donors of convalescent plasma were between the ages
of 18 and 60 years. The donors had recovered from SARS-
CoV-2 infection and were invited to donate their convales-
cent plasma after written informed consent was obtained. All
Methods donors had been previously diagnosed with laboratory-
This study was conducted at the infectious disease depart- confirmed COVID-19 and subsequently tested negative for
ment, Shenzhen Third People's Hospital, Shenzhen, China, SARS-CoV-2 and other respiratory viruses, as well as for
from January 20, 2020, to March 25, 2020, and the final date hepatitis B virus, hepatitis C virus, HIV, and syphilis at the
of follow-up was March 25, 2020. The study was approved by time of blood donation. The donors had been well (asymp-
the ethics committees from Shenzhen Third People’s Hospi- tomatic) for at least 10 days, with a serum SARS-CoV-2–
tal, and each patient gave written informed consent. specific ELISA antibody titer higher than 1:1000 and a neu-
tralizing antibody titer greater than 40. Following donation,
Patients 400 mL of convalescent plasma was obtained from each
Patients with laboratory confirmed COVID-19, diagnosed donor by apheresis, and the plasma was immediately trans-
using quantitative reverse transcriptase–polymerase chain fused to the recipients on the same day it was obtained.
reaction (qRT-PCR) (GeneoDX Co, Ltd) 13 were eligible to
receive convalescent plasma treatment if they fulfilled the Clinical Information
following criteria: (1) had severe pneumonia with rapid pro- Clinical information for the 5 patients before and after conva-
gression and continuously high viral load despite antiviral lescent plasma transfusion was obtained from a review of the
treatment; (2) PAO2/FIO2 of <300 (PAO2 measured in mm Hg and hospital computer medical system and included the follow-
FIO2 measured as fraction of inspired oxygen)14; and (3) were ing: demographic data, days of admission from symptom on-
currently or had been supported with mechanical ventilation. set, and presenting symptoms; data about various treat-
The serum of each recipient was obtained and enzyme-linked ments, including mechanical ventilation, antiviral therapies,
immunosorbent assay (ELISA) and neutralizing antibody titers and steroids; clinical data, including body temperature,
were tested one day prior to the convalescent plasma transfu- PAO2/FIO2, and Sequential Organ Failure Assessment (SOFA)
sion. The ABO blood types of the patients were determined for score (range 0-24, with higher scores indicating more severe
E2 JAMA Published online March 27, 2020 (Reprinted) jama.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma Preliminary Communication Research
illness); laboratory data, including white blood cell count, lym- recipients were obtained on day −1, day 1, day 3, day 7, and day
phocyte count, chemistry panels assessing liver and kidney 12 after the transfusion.
function, cycle threshold value (Ct), inflammatory factors
C-reactive protein (CRP), procalcitonin, and IL-6, and serum ELISA
antibody titer (IgG, IgM, and neutralizing antibodies); data from Microtiter plates (Sangon Biotech) were coated overnight at 4 °C
chest imaging studies; and information on complications, such with 4 μg/mL recombinant SARS-CoV-2 RBD (receptor bind-
as acute respiratory distress syndrome (ARDS), bacterial pneu- ing domain) proteins (50 μL per well) expressed by our labo-
monia, and multiple organ dysfunction syndrome. ratory through 293-T cells. The plates were washed 3 times with
phosphate-buffered saline (PBS) containing 0.1% vol/vol
Quantitative RT-PCR Tween-20 (PBST) and blocked with blocking solution (PBS con-
The qRT-PCR for SARS-CoV-2 was assessed as described taining 2% wt/vol nonfat dry milk) for 2 hours at 37 °C. The
previously.13 Nasopharyngeal specimens collected during hos- plates were then washed with PBST. The serum samples were
pitalization were sent to the laboratory in a viral transport case. diluted to 200-fold into PBS as initial concentration, and se-
Total nucleic acid extraction from the samples was per- rial 3-fold dilutions of serum was added to the wells and in-
formed using the QIAamp RNA Viral Kit (Qiagen), and qRT-PCR cubated at 37 °C for 60 minutes. After 3 washes, 100 μL of
was performed using a commercial kit specific for 2019-nCoV horseradish peroxidase–conjugated goat anti–human IgG
detection (GeneoDX Co) approved by the China Food and Drug (for IgG antibody titer detection) and IgM (for IgM antibody titer
Administration. Each RT-PCR assay provided a Ct value, which detection) antibodies solution (Sangon Biotech) were added
is the number of cycles required for the fluorescent signal to to each plate, respectively, and incubated at 37 °C for 60 min-
cross the threshold for a positive test: a higher Ct value is cor- utes. After 5 washes, 100 μL of tetramethylbenzidine sub-
related with a lower viral load. The specimens were consid- strate (Sangon Biotech) was added at room temperature in
ered positive if the Ct value was 37.0 or lower and negative if the dark. After 15 minutes, the reaction was stopped with
the results were undetermined. Specimens with a Ct value a 2 M H2SO4 solution (sulfuric acid). The absorbance was mea-
higher than 37 were repeated. The specimen was considered sured at 450 nm. All samples were run in triplicate. The ELISA
positive if the repeated results were the same as the initial re- titers were determined by end point dilution.
sult and between 37 and 40. If the repeated Ct was undetect-
able, the specimen was considered negative. All procedures Serum Neutralization Assay
involving clinical specimens and SARS-CoV-2 were per- Vero cells (104) were seeded 24 hours before the infection in a
formed in a biosafety level 3 laboratory. The Ct values of the 5 96-well plate (Costar). On the day of infection, the cells were
Table 1. Clinical Characteristics of SARS-CoV-2-Infected Patients Who Received Convalescent Plasma
Patient
1 2 3 4 5
Sex Male Male Female Female Male
Age, y 70s 60s 50s 30s 60s
Weight, kg 55 85 60 41.5 87
Smoking No No No No No
Blood type B B B A B
Coexisting chronic diseases None Hypertension; mitral None None None
insufficiency
Disease presentation and course
Estimated incubation period, da 1 7 3 7 15
Interval between symptom onset 2 4 2 2 3
and admission, d
Interval between admission 22 10 20 19 20
and plasma transfusion, d
Complications prior to plasma Bacterial Bacterial pneumonia; Severe ARDS Severe ARDS Severe ARDS
transfusion pneumonia; severe fungal pneumonia;
ARDS; MODS severe ARDS;
myocardial damage
Most severe disease classification Critical Critical Critical Critical Critical
Treatments
Steroids Methylprednisolone Methylprednisolone Methylprednisolone Methylprednisolone Methylprednisolone
Antivirals Lopinavir/ritonavir; Lopinavir/ritonavir; Lopinavir/ritonavir; Interferon alfa-1b; Lopinavir/ritonavir;
interferon alfa-1b; arbidol; darunavir interferon alfa-1b; favipiravir interferon alfa-1b
favipiravir
a
Abreviations: ARDS, acute respiratory distress syndrome; MODS, multiple organ Estimated incubation period defined as interval between estimated exposure
dysfunction syndrome; SARS-CoV-2, severe acute respiratory syndrome to SARS-CoV-2 and symptom onset.
coronavirus 2.
jama.com (Reprinted) JAMA Published online March 27, 2020 E3
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Research Preliminary Communication Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma
Table 2. Comparison of Viral Load, Clinical Indexes, and Laboratory Results Before and After
Convalescent Plasma Transfusion
Patient
1 2 3 4 5
Clinical characteristics
Body temperature, °C
Just before transfusion 38.6 39.0 37.6 38.3 39.0
Day 1 posttransfusion 38.5 36.8 37.7 37.9 39.0
Day 3 posttransfusion 38.1 36.6 37.0 36.6 36.8
Day 7 posttransfusion 37.8 37.2 36.5 37.9 36.8
Day 12 posttransfusion 37.0 36.8 36.6 36.8 37.9
SOFA scorea
Just before transfusion 5 10 3 3 2
Day 1 posttransfusion 4 12 4 3 2
Day 3 posttransfusion 6 10 3 2 2
Day 5 posttransfusion 5 11 2 2 2
Day 7 posttransfusion 3 7 2 2 1
Day 12 posttransfusion 2 4 2 1 1
PAO2/FIO2b
Just before transfusion 276 209 172 188 205
Day 1 posttransfusion 300 134 184 242 292
Day 3 posttransfusion 220 230 164 233 304
Day 7 posttransfusion 245 206 220 290 230
Day 12 posttransfusion 284 316 342 322 366
Ct valuec (viral load proxy)
On admission to hospital 23.0 19.7 18.9 38.0 28.0
Lowest value during hospitalizationd 19.2 19.7 18.9 26.6 26.5
(highest viral load)
Just before plasma transfusion 28.5 22.0 33.0 26.6 35.9
Day 1 posttransfusion 30.0 23.7 38.5 28.0 Negative
Day 3 posttransfusion 34.4 25.0 Negative Negative Negative
Day 7 posttransfusion 38.0 32.0 Negative Negative Negative
Day 12 posttransfusion Negative Negative Negative Negative Negative
Mechanical ventilation
Onset, days before transfusion 11 2 12 9 2
Extubated, days posttransfusion Intubated Intubated 2 9 9
ECMO
Onset, days before transfusion Not received 1 Not received Not received Not received
Removal, days posttransfusion NA 5 NA NA NA
Laboratory findings
C-reactive protein, mg/L (normal range, <8)
Before transfusion 163.4 242.8 65. 156.0 173.1
Day 1 posttransfusion 146.2 223.0 108.3 NT 186.8
Day 3 posttransfusion 115.1 75.2 78.7 160.8 233.7
Day 5 posttransfusion 31.3 10.4 74.7 NT 260.4
Day 7 posttransfusion 31.2 13.9 6.2 9.6 5.5
Day 12 posttransfusion 5.3 33.1 NT 5.8 3.2
Procalcitonin, ng/mL (normal range, <0.1)
Before transfusion 1.2 7.3 0.1 0.2 0.2
Day 1 posttransfusion 1.3 19.7 0.1 0.08 0.4
Day 3 posttransfusion 1.6 13.9 0.09 0.07 1.5
Day 5 posttransfusion 0.9 1.8 0.08 NT 0.9
Day 7 posttransfusion 1.1 0.1 0.04 0.04 0.09
Day 12 posttransfusion 0.4 0.2 NT 0.04 0.07
(continued)
E4 JAMA Published online March 27, 2020 (Reprinted) jama.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma Preliminary Communication Research
Table 2. Comparison of Viral Load, Clinical Indexes, and Laboratory Results Before and After
Convalescent Plasma Transfusion (continued)
Patient
1 2 3 4 5
IL-6, pg/mL (normal range, 0-7)
Before transfusion 70.5 438.2 63.9 79.1 87.8
Day 1 posttransfusion 74.9 NT 118.5 39.3 NT
Day 3 posttransfusion 34.5 1045.0 67.0 25.8 797.9
Day 5 posttransfusion 24.1 334.1 590.5 NT NT
Day 7 posttransfusion 30.8 29.8 174.3 34.0 69.9
Day 12 posttransfusion 6.1 31.8 NT 2.7 54.9
Length of hospital stay, d Remains Remains 53 51 55
hospitalized hospitalized
Current status as of March 25, 2020 Stable, still Stable, still Discharged Discharged Discharged
receiving receiving home home home
mechanical mechanical
ventilation ventilation
Abbreviations: Ct, cycle threshold; ECMO, extracorporeal membrane oxygenation; NT, not tested.
a
The SOFA score is calculated using 6 systems: respiratory, coagulation, hepatic, cardiovascular, central nervous system,
and kidney. A score of 0 is given for normal function through to 4 for most abnormal for each system. The worst values
on each day are recorded, and the final SOFA score is the sum of the scores of each system.
b
PAO2/FIO2 ratio was defined as the ratio of the partial pressure of arterial oxygen to the percentage of inspired oxygen.
c
Cycle threshold is the number of polymerase chain reaction cycles required for gene amplification. A higher Ct value is
correlated with a lower viral load.
d
Lowest value (highest viral load) between hospital admission and plasma transfusion.
washed twice. Serum samples from patients were incubated The SOFA score ranged from 2 to 10 prior to plasma trans-
at 56 °C for 30 minutes and then diluted 2-fold in cell culture fusion, and decreased to a range of 1 to 4 at 12 days following
medium (modified eagle medium). Aliquots (40 μL) of di- transfusion (Table 2 and Figure 1B). The PAO2/FIO2 ranged from
luted serum samples (from 2-fold to 2056-fold) were added to 172 to 276 prior to transfusion, and increased (improved) for
50 μL of cell culture medium containing 50 times the tissue 4 of 5 patients within 7 days after transfusion (overall range,
culture infective dose (TCID50) of the BetaCoV/Shenzhen/ 206-290), and increased substantially (range, 284-366) on the
SZTH-003/2020 strain virus (isolated from this hospital, GI- 12th day after the plasma treatment (Table 2 and Figure 1C).
SAID access number: EPI_ISL_406594)15 on a 96-well plate and Body temperature ranged from 37.6 to 39.0 °C before plasma
incubated at 37 °C for 2 hours in CO2 5% vol/vol. Virus anti- transfusion and declined to the normal range on the third day
body mix was then added to cells in 96-well plates and plates after the transfusion (Table 2 and Figure 1D).
were incubated at 37 °C with microscopic examination for cy- After the treatment, the values of the inflammatory bio-
topathic effect after a 5-day incubation. The highest dilution markers CRP, procalcitonin, and IL-6 of patients 1, 2, 4, and 5
of serum that showed inhibition activity of SARS-CoV-2 was decreased; the values of CRP and procalcitonin of patient 3 de-
recorded as the neutralizing antibody titer. Assays were per- creased (Table 2).
formed in triplicate with negative control samples from healthy The computed tomography scans of the lungs of these pa-
volunteers. tients all demonstrated severe pneumonia prior to plasma
transfusion and showed improvement of the pulmonary le-
sion of patient 1 on the third day after the plasma transfusion
(eFigure 1 in the Supplement) and gradual resolution of pul-
Results monary lesions of other patients at 3 days after the plasma treat-
Five patients (age range, 36-73 years; 2 women) were treated ment (eFigures 2, 3, 4, and 5 in the Supplement).
with convalescent serum. None were smokers, and 4 of 5 had One day prior to convalescent plasma administration, the
no preexisting medical conditions. All 5 had received various RBD-specific IgG and IgM ELISA titers of the donors ranged be-
antiviral agents and steroids (Table 1). Convalescent plasma was tween 1800 and 16 200 (ELISA end point dilution titers)
administered between 10 and 22 days after admission. (Table 3). The neutralization titers against SARS-CoV-2 ranged
The Ct value at the time of admission ranged from 18.9 to between 80 and 480 (neutralizing end point dilution titers).
38.0, and on the day of plasma transfusion from 22.0 to 35.9 The RBD-specific IgG ELISA titers of 5 recipients ranged be-
(Table 2 and Figure 1A). It increased (improved) within 1 day tween 1800 and 48 600 and the IgM titers between 5400 and
after transfusion. The Ct value of patient 5 became negative 145 800 a day prior to the convalescent transfusion (eTable in
on posttransfusion day 1, patient 3 and patient 4 became nega- the Supplement). After the transfusion of convalescent plasma,
tive on day 3, and patient 1 and patient 2 became negative on the titers of IgG and IgM in the sera of these patients in-
day 12 after the transfusion (Table 2). creased in a time-dependent manner. The IgG titers of the
jama.com (Reprinted) JAMA Published online March 27, 2020 E5
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Research Preliminary Communication Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma
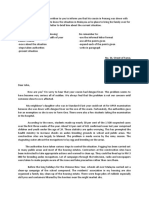
Figure 1. Temporal Changes of Cycle Threshold Value, PAO2/FIO2, SOFA Score, and Body Temperature in Patients Receiving
Convalescent Plasma Transfusion
A Cycle threshold B SOFA score
45 15
Patients
40 1
2
3
10
4
SOFA score
35
5
Ct value
30
5
25
20 0
0 1 3 7 12 0 1 3 7 12
Days posttransfusion Days posttransfusion
C PAO2/FIO2 D Body temperature
400 40
Body temperature, °C 39
300
PAO2/FIO2
38
200
37
100 36
0 1 3 7 12 0 1 3 7 12
Days posttransfusion Days posttransfusion
A, Change in cycle threshold (Ct) value in nasopharyngeal swabs of infected (range 0-24, with higher scores indicating more severe illness; see footnote to
patients at day 0, day 3, day 7, and day 12 after the plasma transfusion. A Ct value Table 2 for more complete definition). C, Change in PAO2/FIO2 ratio of the treated
of 40 was defined as undetectable. B, Change in Sequential Organ Failure patients from day 0 to day 12 after treatment. D, Change in body temperature of
Assessment (SOFA) score of the patients with convalescent plasma treatment the 5 patients following plasma transfusion.
Table 3. Characteristics and Antibody Titer of Convalescent Plasma Donors
Donorsa
1 2 3 4 5
Blood type B B B A B
Donated plasma volume, mL 400 400 400 400 400
Interval between symptom onset and discharge, d 11 11 13 13 11
Interval between discharge and plasma donation, d 11 11 13 11 12
RBD-specific IgG ELISA titerb 16 200 1800 1800 5400 16 200
RBD-specific IgM ELISA titerc 16 200 1800 5400 5400 5400
Neutralizing antibody titerd 240 80 120 240 480
c
Abbreviation: RBD, receptor binding domain. ELISA end point dilution titers (IgM antibody). The expected titer of negative
a
Donors-patients were matched by number (donor 1 gave plasma to control from a healthy person is ⱕ200.
d
patient 1, etc). Neutralization end point dilution titers. The expected titer of negative control
b
ELISA end point dilution titers (IgG antibody). The expected titer of negative from a healthy person is ⱕ10.
control from a healthy person is ⱕ200.
treated patients increased to 145 800, 5400, 5400, 145 800 and sion. These IgG and IgM titers maintained a high level at 7 days
145 800, and the IgM titers increased to 145 800, 5400, 5400, after transfusion (Figure 2A and 2B; eTable in the Supple-
437 400 and 145 800, respectively, at 3 days after transfu- ment). The neutralizing antibody titers of the 5 recipients
E6 JAMA Published online March 27, 2020 (Reprinted) jama.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma Preliminary Communication Research
Figure 2. Changes of Receptor Binding Domain–Specific IgG and IgM ELISA and Neutralizing Antibody Titers Before and After
Convalescent Plasma Transfusion in Patients
Patients
1
2
A RBD-specific IgG ELISA titer B RBD-specific IgM ELISA titer C Neutralizing antibody titer 3
4
150 150 1000
IgM ELISA titer, in thousands
5
IgG ELISA titer, in thousands
Neutralizing antibody titer
100 100
100
10 10
1 1 10
0 1 3 7 0 1 3 7 0 1 3 7
Days posttransfusion Days posttransfusion Days posttransfusion
Higher titer values indicate greater protection. A, Variation of RBD-specific IgG day 3, and day 7 following transfusion. The identical line segments were
ELISA titer. B, Variation of RBD-specific IgM ELISA titer. C, Variation of adjusted slightly to avoid superimposition. RBD indicates receptor binding
neutralizing antibody titer against SARS-CoV-2 in recipients in day 0, day 1, domain.
ranged between 40 and 160 before transfusion; one day after had significantly fewer deaths (20% vs 54.8%; P = .01) and
transfusion, the titers increased to 320, 80, 80, 160, and 240; a lower median lymphocyte count on ICU admission.10
on day 7, they were 320, 160, 160, 240, and 480, respectively In this study, collection and transfusion of the plasma
(Figure 2C; eTable in the Supplement). were done as previously reported.10 In addition, plasma was
All 5 patients were receiving mechanical ventilation at obtained from the donors and transfused in the recipients
the time of transfusion, and 3 patients (patients 3, 4, and 5) on the same day, which helps preserve the natural activity of
were weaned from mechanical ventilation (Table 2). Patient 2 the plasma.
was receiving ECMO at the time of plasma treatment but did Studies have shown that viral loads are highly correlated
not require ECMO on day 5 after transfusion (Table 2). with disease severity and progression.18 Fatal outcome of hu-
Patients 3, 4, and 5 were discharged from the hospital (length man influenza A(H5N1) has been associated with high viral load
of stay: 53, 51, and 55 days, respectively). As of March 25, and hypercytokinemia.19 Apart from antiviral treatment, virus-
2020, patients 1 and 2 remained hospitalized, with lengths of specific neutralizing antibody, which could accelerate virus
stay of 37 days each. clearance and prevent entry into target cells, serves as the main
mechanism for the restriction and clearance of the viruses by
the host.20-22 In the current study, SARS-CoV-2 was still detect-
able in all 5 patents even though antiviral treatment had been
Discussion given for at least 10 days, although viral load decreased and be-
In this case series, 5 patients who were critically ill with came undetectable soon after convalescent plasma treatment.
COVID-19 were treated with convalescent plasma. As As determined by ELISA, all plasma from the donors had high
assessed by Ct, viral load declined within days of treatment virus-specific IgG and IgM ELISA titers. Moreover, the neutral-
with convalescent plasma, and the clinical conditions of izing antibody titers, vital for the restriction of viral infection
these patients improved, as indicated by body temperature of the 5 recipients, significantly increased after plasma trans-
reduction, improved P AO 2 /F IO 2 , and chest imaging. Four fusion. The results highlight the possibility that antibodies from
patients who had been receiving mechanical ventilation and convalescent plasma may have contributed to the clearance of
ECMO no longer required respiratory support by 9 days after the virus and also the improvement of symptoms. In addition
plasma transfusion. to viral neutralizing antibodies, acceleration of infected cell
Previous studies have reported the use of convalescent clearance by antibodies has also been found in an in vivo study
plasma transfusion in the treatment of various infections.6,10,16 of HIV-1 virus.23 In the current study, all patients received an-
For example, patients (n = 50) with SARS had a significantly tiviral agents, including interferon and lopinavir/ritonavir, dur-
higher discharge rate by day 22 following onset of illness (73.4% ing and following convalescent plasma treatment, which also
vs 19.0%; P<.001) and lower case-fatality rate (0% vs 23.8%; may have contributed to the viral clearance observed.
P = .049) in the convalescent plasma treatment group (n = 19
patients) when compared with steroid treatment group Limitations
(n = 21).17 In another study of 93 patients with influenza This study has several limitations. First, this was a small case
A(H1N1), patients who received convalescent plasma treat- series that included no controls. Second, it is unclear if these
ment (n = 20) compared with those in the control group (n = 73) patients would have improved without transfusion of
jama.com (Reprinted) JAMA Published online March 27, 2020 E7
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Research Preliminary Communication Treatment of Critically Ill Patients With COVID-19 With Convalescent Plasma
convalescent plasma, although the change in Ct and PAO2/
FIO2 represent encouraging findings. Third, all patients were Conclusions
treated with multiple other agents (including antiviral medi-
cations), and it is not possible to determine whether the im- In this preliminary uncontrolled case series of 5 critically ill pa-
provement observed could have been related to therapies other tients with COVID-19 and ARDS, administration of convales-
than convalescent plasma. Fourth, plasma transfusion was ad- cent plasma containing neutralizing antibody was followed by
ministered 10 to 22 days after admission; whether a different improvement in the patients’ clinical status. The limited sample
timing of administration would have been associated with dif- size and study design preclude a definitive statement about
ferent outcomes cannot be determined. Fifth, whether this ap- the potential effectiveness of this treatment, and these obser-
proach would reduce case-fatality rates is unknown. vations require evaluation in clinical trials.
ARTICLE INFORMATION Role of the Funder/Sponsor: The funding agencies 13. Yang Y, Yang M, Shen C, et al Evaluating the
Accepted for Publication: March 20, 2020. had no role in the design and conduct of the study; accuracy of different respiratory specimens in the
collection, management, analysis, and laboratory diagnosis and monitoring the viral
Published Online: March 27, 2020. interpretation of the data; preparation, review, or shedding of 2019-nCoV infections. Preprint.
doi:10.1001/jama.2020.4783 approval of the manuscript; and decision to submit medRxiv. Preprint posted online February 17, 2020.
Author Affiliations: Shenzhen Key Laboratory of the manuscript for publication. doi:10.1101/2020.02.11.20021493
Pathogen and Immunity, National Clinical Research 14. Villar J, Blanco J, del Campo R, et al; Spanish
Center for Infectious Disease, State Key Discipline REFERENCES Initiative for Epidemiology, Stratification &
of Infectious Disease, Shenzhen Third People's 1. Huang C, Wang Y, Li X, et al. Clinical features of Therapies for ARDS (SIESTA) Network. Assessment
Hospital, Second Hospital Affiliated to Southern patients infected with 2019 novel coronavirus in of PaO2/FiO2 for stratification of patients with
University of Science and Technology, Shenzhen, Wuhan, China. Lancet. 2020;395(10223):497-506. moderate and severe acute respiratory distress
China (Shen, Z. Wang, Zhao, Y. Yang, J. Li, Yuan, syndrome. BMJ Open. 2015;5(3):e006812. doi:10.
F. Wang, D. Li, M. Yang, Xing, Wei, Xiao, Y. Yang, Qu, 2. WHO. Novel coronavirus (COVID-19) situation.
Updated March 24, 2020. https://experience. 1136/bmjopen-2014-006812
Qing, L. Chen, Xu, Peng, Y. Li, Zheng, F. Chen,
Huang, Jiang, D. Liu, Zhang, Y. Liu, L. Liu); arcgis.com/experience/ 15. Liu C, Yang Y, Gao Y, et al Viral architecture of
Laboratory of Protein Engineering and Vaccines, 685d0ace521648f8a5beeeee1b9125cd SARS-CoV-2 with post-fusion spike revealed by
Tianjin Institute of Industrial Biotechnology, 3. Wu Z, McGoogan JM. Characteristics of and Cryo-EM. bioRxiv. Preprint posted online March 5,
Chinese Academy of Sciences (CAS), Tianjin, China important lessons from the coronavirus disease 2020. doi:10.1101/2020.03.02.972927
(D. Li, Xiao). 2019 (COVID-19) outbreak in China: summary of a 16. Yeh KM, Chiueh TS, Siu LK, et al. Experience of
Author Contributions: Dr L. Liu had full access to report of 72 314 cases from the Chinese Center for using convalescent plasma for severe acute
all of the data in the study and takes responsibility Disease Control and Prevention. JAMA. 2020. respiratory syndrome among healthcare workers in
for the integrity of the data and the accuracy of the Published online February 24, 2020. doi:10.1001/ a Taiwan hospital. J Antimicrob Chemother. 2005;
data analysis. Drs Shen, Z. Wang, Zhao, and Y. Yang jama.2020.2648 56(5):919-922.
contributed equally. 4. LuH.Drugtreatmentoptionsforthe2019-newcoro- 17. Mair-Jenkins J, Saavedra-Campos M, Baillie JK,
Concept and design: Shen, Z. Wang, Yuan, F. Wang, navirus (2019-nCoV). Biosci Trends. 2020;14(1):69-71. et al; Convalescent Plasma Study Group. The
D. Liu, Zhang, Y. Liu, L. Liu. 5. Chen L, Xiong J, Bao L, Shi Y. Convalescent effectiveness of convalescent plasma and
Acquisition, analysis, or interpretation of data: Shen, plasma as a potential therapy for COVID-19. Lancet hyperimmune immunoglobulin for the treatment of
Yang Yang, J. Li, Yuan, D. Li, M. Yang, Xing, Wei, Infect Dis. 2020;S1473-3099(20)30141-9. severe acute respiratory infections of viral etiology:
Xiao, Yan Yang, Qu, Qing, L. Chen, Xu, Peng, Y. Li, a systematic review and exploratory meta-analysis.
Zheng, F. Chen, Huang, Jiang, Y. Liu, L. Liu. 6. Kraft CS, Hewlett AL, Koepsell S, et al; Nebraska J Infect Dis. 2015;211(1):80-90.
Drafting of the manuscript: Shen, Zhao, Yang Yang, Biocontainment Unit and the Emory Serious
Communicable Diseases Unit. The use of 18. Ng KT, Oong XY, Lim SH, et al. Viral load and
J. Li, Yuan, F. Wang, M. Yang, Xing, Wei, Xiao, Yan sequence analysis reveal the symptom severity,
Yang, Qu, Qing, L. Chen, Xu, Zheng, Huang, Jiang, TKM-100802 and convalescent plasma in 2
patients with Ebola virus disease in the United diversity, and transmission clusters of rhinovirus
D. Liu, Y. Liu, L. Liu. infections. Clin Infect Dis. 2018;67(2):261-268.
Critical revision of the manuscript for important States. Clin Infect Dis. 2015;61(4):496-502.
intellectual content: Shen, Z. Wang, Yang Yang, 7. van Griensven J, Edwards T, de Lamballerie X, 19. de Jong MD, Simmons CP, Thanh TT, et al. Fatal
Yuan, D. Li, Peng, Y. Li, F. Chen, Zhang, Y. Liu, L. Liu. et al; Ebola-Tx Consortium. Evaluation of outcome of human influenza A (H5N1) is associated
Statistical analysis: Yuan. convalescent plasma for Ebola virus disease in with high viral load and hypercytokinemia. Nat Med.
Obtained funding: Yuan, Zhang, Y. Liu, L. Liu. Guinea. N Engl J Med. 2016;374(1):33-42. 2006;12(10):1203-1207.
Administrative, technical, or material support: Shen, 8. Florescu DF, Kalil AC, Hewlett AL, et al. 20. Shen C, Chen J, Li R, et al. A multimechanistic
Zhao, J. Li, Yuan, F. Wang, D. Li, M. Yang, Yan Yang, Administration of brincidofovir and convalescent antibody targeting the receptor binding site
Qu, Qing, L. Chen, Zhang. plasma in a patient with Ebola virus disease. Clin potently cross-protects against influenza B viruses.
Supervision: Z. Wang, Yuan, Zhang, Y. Liu, L. Liu. Infect Dis. 2015;61(6):969-973. Sci Transl Med. 2017;9(412):eaam5752.
Conflict of Interest Disclosures: None reported. 9. Zhou B, Zhong N, Guan Y. Treatment with 21. Shen C, Zhang M, Chen Y, et al. An IgM antibody
Funding/Support: This work was supported by the convalescent plasma for influenza A (H5N1) targeting the receptor binding site of influenza B
National Science and Technology Major Project infection. N Engl J Med. 2007;357(14):1450-1451. blocks viral infection with great breadth and
(2018ZX10711001, 2017ZX10103011, potency. Theranostics. 2019;9(1):210-231.
10. Hung IF, To KK, Lee CK, et al. Convalescent
2017ZX10204401), Sanming Project of Medicine in plasma treatment reduced mortality in patients 22. Wang C, Li W, Drabek D, et al A human
Shenzhen (SZSM201412003, SZSM201512005), with severe pandemic influenza A (H1N1) 2009 monoclonal antibody blocking SARS-CoV-2
China Postdoctoral Science Foundation virus infection. Clin Infect Dis. 2011;52(4):447-456. infection. bioRxiv. Preprint posted online March 12,
(2019T120147, 2018M641508), Shenzhen Science 2020. doi:10.1101/2020.03.11.987958
and Technology Research and Development Project 11. Burnouf T, Radosevich M. Treatment of severe
acute respiratory syndrome with convalescent 23. Lu CL, Murakowski DK, Bournazos S, et al.
(202002073000001), National Natural Science Enhanced clearance of HIV-1-infected cells by
Foundation of China (81902058), Shenzhen Science plasma. Hong Kong Med J. 2003;9(4):309.
broadly neutralizing antibodies against HIV-1 in vivo.
and Technology Research and Development Project 12. Cheng Y, Wong R, Soo YO, et al. Use of Science. 2016;352(6288):1001-1004.
(202002073000002), and The Key Technology convalescent plasma therapy in SARS patients in
R&D Program of Tianjin (17YFZCSY01090). Hong Kong. Eur J Clin Microbiol Infect Dis. 2005;24
(1):44-46.
E8 JAMA Published online March 27, 2020 (Reprinted) jama.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Johns Hopkins University User on 03/27/2020
Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- 2017 ESMO Essentials For Clinicians Gynaecological TumoursDocumento100 pagine2017 ESMO Essentials For Clinicians Gynaecological TumoursMaria RamosNessuna valutazione finora
- Testing The SF-36 in Parkinson's Disease: Implications For Reporting Rating Scale DataDocumento9 pagineTesting The SF-36 in Parkinson's Disease: Implications For Reporting Rating Scale DataMaria RamosNessuna valutazione finora
- Testing The SF-36 in Parkinson's Disease: Implications For Reporting Rating Scale DataDocumento9 pagineTesting The SF-36 in Parkinson's Disease: Implications For Reporting Rating Scale DataMaria RamosNessuna valutazione finora
- Pain in Parkinson's Disease: Blair Ford, MDDocumento6 paginePain in Parkinson's Disease: Blair Ford, MDMaria RamosNessuna valutazione finora
- Chaudhuri 2010Documento6 pagineChaudhuri 2010Maria RamosNessuna valutazione finora
- The Meaning in Quality of LifeDocumento3 pagineThe Meaning in Quality of LifeMaria RamosNessuna valutazione finora
- Nonmotor Disturbances in Parkinson's Disease: DiseasesDocumento14 pagineNonmotor Disturbances in Parkinson's Disease: DiseasesMaria RamosNessuna valutazione finora
- PD Awareness Week - Map Launch - 16 - 04 - 2012Documento2 paginePD Awareness Week - Map Launch - 16 - 04 - 2012Maria RamosNessuna valutazione finora
- Neuropsychiatric Symptoms in Parkinson's Disease: ReviewDocumento9 pagineNeuropsychiatric Symptoms in Parkinson's Disease: ReviewMaria RamosNessuna valutazione finora
- Sleep DisordersDocumento4 pagineSleep DisordersMaria RamosNessuna valutazione finora
- Presentation 1Documento2 paginePresentation 1Maria RamosNessuna valutazione finora
- Report On Students Activity During ClassesDocumento1 paginaReport On Students Activity During ClassesMaria RamosNessuna valutazione finora
- Business PPT TemplateDocumento4 pagineBusiness PPT TemplateMaria RamosNessuna valutazione finora
- Business TemplateDocumento4 pagineBusiness TemplateMaria RamosNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 2018 MTE GIVD Classification 2018 Rev01Documento14 pagine2018 MTE GIVD Classification 2018 Rev01Dr.Sivakumar SelvarajNessuna valutazione finora
- Fe310 Food Technology 3rd WeekDocumento29 pagineFe310 Food Technology 3rd Weekirem emine demirNessuna valutazione finora
- PMD, A Registered Botanical Mosquito Repellent With Deet-Like Efficacy - PubMedDocumento1 paginaPMD, A Registered Botanical Mosquito Repellent With Deet-Like Efficacy - PubMedG TNessuna valutazione finora
- Harga TindakanDocumento494 pagineHarga TindakanIndera KesumaNessuna valutazione finora
- AntigenDocumento29 pagineAntigenSarhad MusaNessuna valutazione finora
- Short Story COVID-19Documento3 pagineShort Story COVID-19Kim SaysonNessuna valutazione finora
- EPA Registered Hard Surface Disinfectants Comparison ChartDocumento7 pagineEPA Registered Hard Surface Disinfectants Comparison ChartPariseerNessuna valutazione finora
- Krishna Prasad ChaliseDocumento1 paginaKrishna Prasad ChaliseChalise SupremeNessuna valutazione finora
- Hepatitis Viruses: Group 3 - MLS 3CDocumento10 pagineHepatitis Viruses: Group 3 - MLS 3CYelai CarveroNessuna valutazione finora
- Oxoid - SdaDocumento1 paginaOxoid - SdaDidik PrasetyaNessuna valutazione finora
- Animal Health Sanitation and Disease Control PathogenDocumento76 pagineAnimal Health Sanitation and Disease Control PathogenKysess OrdinarioNessuna valutazione finora
- A Antimicrobial Susceptibility TestingDocumento13 pagineA Antimicrobial Susceptibility TestingkurfaNessuna valutazione finora
- Diseases of SilkwormDocumento11 pagineDiseases of Silkwormbashirlone786Nessuna valutazione finora
- Quiz navigation: Home Courses 2018 يوﯾطﻌﻟا ﻲﻧﯾﺳﺣﻟا دوﻣﺣﻣ ﮫﻣﺣر "Documento31 pagineQuiz navigation: Home Courses 2018 يوﯾطﻌﻟا ﻲﻧﯾﺳﺣﻟا دوﻣﺣﻣ ﮫﻣﺣر "Rahma MahmouuddNessuna valutazione finora
- Department of Genetics: Rapid Antigen Test - Covid 19Documento1 paginaDepartment of Genetics: Rapid Antigen Test - Covid 19Liya Mary VargheseNessuna valutazione finora
- VIRUSESDocumento21 pagineVIRUSESSome BodyNessuna valutazione finora
- Malaria: Potrait of A DeseaseDocumento1 paginaMalaria: Potrait of A DeseaseAcap SkylunkNessuna valutazione finora
- Vagina TrichomoniasisDocumento46 pagineVagina Trichomoniasissachikoroseate75% (4)
- Al3177hv Al3177 3091280Documento14 pagineAl3177hv Al3177 3091280JimmyNessuna valutazione finora
- Article-2021-COVID-19-Neutralizing Antibodies Predict Disease Severity and SurvivalDocumento25 pagineArticle-2021-COVID-19-Neutralizing Antibodies Predict Disease Severity and Survivalcarlos ArozamenaNessuna valutazione finora
- Office Hygiene British English Upper Intermediate Advanced GroupDocumento3 pagineOffice Hygiene British English Upper Intermediate Advanced GroupPablo Tejedor LópezNessuna valutazione finora
- Resistance Is Futile ... or Is It?: The Immune System and HIV InfectionDocumento28 pagineResistance Is Futile ... or Is It?: The Immune System and HIV InfectionRachel Mwale MwazigheNessuna valutazione finora
- Robert Kennedy, JR.: "The Government Has Been Trying For AlmostDocumento3 pagineRobert Kennedy, JR.: "The Government Has Been Trying For AlmostjayjonbeachNessuna valutazione finora
- Effect of Antibiotic On BacteriaDocumento19 pagineEffect of Antibiotic On BacteriaTootsie100% (2)
- Research in Social and Administrative PharmacyDocumento4 pagineResearch in Social and Administrative PharmacyAndrea MendozaNessuna valutazione finora
- ActinomycosisDocumento26 pagineActinomycosistummalapalli venkateswara rao100% (1)
- Lifebuoy 120324115017 Phpapp02Documento38 pagineLifebuoy 120324115017 Phpapp02Binush ThampanNessuna valutazione finora
- Pathogenic Mechanisms of HIV Disease: FurtherDocumento28 paginePathogenic Mechanisms of HIV Disease: FurtherSefren TumilaarNessuna valutazione finora
- Informal Letter DengueDocumento2 pagineInformal Letter DengueIrsyad IzzatNessuna valutazione finora
- Topic 1 - Principles of ImmunologyDocumento2 pagineTopic 1 - Principles of ImmunologyKim Alyssa GoNessuna valutazione finora