Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Ultrasound Spectrum in Intraductal Papillary Neoplasms of BreastDocumento7 pagineUltrasound Spectrum in Intraductal Papillary Neoplasms of BreastdrrahulsshindeNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Tubeless Hypotonic DuodenographyDocumento12 pagineTubeless Hypotonic DuodenographydrrahulsshindeNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Surgical Anatomy PF PNSDocumento11 pagineSurgical Anatomy PF PNSdrrahulsshindeNessuna valutazione finora
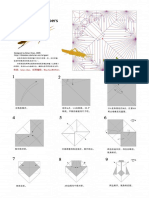
- Brian Chan-Locust PDFDocumento10 pagineBrian Chan-Locust PDFdrrahulsshindeNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Frontal Sinus Drainage Pathway PDFDocumento9 pagineFrontal Sinus Drainage Pathway PDFdrrahulsshindeNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Quarterly Oru Folding Diagrams - Vol.2Documento186 pagineQuarterly Oru Folding Diagrams - Vol.2drrahulsshinde89% (19)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Quarterly Oru Folding Diagrams Vol 1Documento199 pagineQuarterly Oru Folding Diagrams Vol 1drrahulsshinde95% (20)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Chi - Square Test: PG Students: DR Amit Gujarathi DR Naresh GillDocumento32 pagineChi - Square Test: PG Students: DR Amit Gujarathi DR Naresh GillNaresh GillNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 24.2 The Core Assumptions of MindfulnessDocumento9 pagine24.2 The Core Assumptions of Mindfulnessale alvarezNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Thorley Amended Complaint (Signed)Documento13 pagineThorley Amended Complaint (Signed)Heather ClemenceauNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Complement Fixation Test: Process Testing For Antigen Semi-Quantitative Testing References External LinksDocumento2 pagineComplement Fixation Test: Process Testing For Antigen Semi-Quantitative Testing References External LinksYASMINANessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Sebaran Populasi Dan Klasifikasi Resistensi Eleusine Indica Terhadap Glifosat Pada Perkebunan Kelapa Sawit Di Kabupaten Deli SerdangDocumento7 pagineSebaran Populasi Dan Klasifikasi Resistensi Eleusine Indica Terhadap Glifosat Pada Perkebunan Kelapa Sawit Di Kabupaten Deli SerdangRiyo RiyoNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Group 5 - Ethical PrinciplesDocumento11 pagineGroup 5 - Ethical Principlesvirgo paigeNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Essay 31 - Permissive ParentingDocumento2 pagineEssay 31 - Permissive Parentingqbich37Nessuna valutazione finora
- G.R. No. 178741Documento1 paginaG.R. No. 178741Jefferson BagadiongNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- ECC83/12AX7: Quick Reference DataDocumento4 pagineECC83/12AX7: Quick Reference DataLuisNessuna valutazione finora
- Hubungan Body Image Dengan Pola Konsumsi Dan Status Gizi Remaja Putri Di SMPN 12 SemarangDocumento7 pagineHubungan Body Image Dengan Pola Konsumsi Dan Status Gizi Remaja Putri Di SMPN 12 SemarangNanda MaisyuriNessuna valutazione finora
- Literary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Documento6 pagineLiterary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Pedro PorbénNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- DR Hoon Park III - Indigenous Microorganism (IMO)Documento33 pagineDR Hoon Park III - Indigenous Microorganism (IMO)neofrieda79100% (1)
- c3175492 Pavan Kumarvasudha Signed OfferletterDocumento6 paginec3175492 Pavan Kumarvasudha Signed OfferletterPavan Kumar Vasudha100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Mdp36 The EndDocumento42 pagineMdp36 The Endnanog36Nessuna valutazione finora
- Buss 37 ZemaljaDocumento50 pagineBuss 37 ZemaljaOlga KovacevicNessuna valutazione finora
- Issue of HomosexualityDocumento4 pagineIssue of HomosexualityT-2000Nessuna valutazione finora
- Figure 1: Basic Design of Fluidized-Bed ReactorDocumento3 pagineFigure 1: Basic Design of Fluidized-Bed ReactorElany Whishaw0% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- BR Interlock Pallet Racking System 2009 enDocumento8 pagineBR Interlock Pallet Racking System 2009 enMalik Rehan SyedNessuna valutazione finora
- Menu Siklus RSDocumento3 pagineMenu Siklus RSChika VionitaNessuna valutazione finora
- Improving The Livelihoods of Smallholder Fruit Farmers in Soroti District, Teso Sub Region, Eastern Uganda RegionDocumento2 pagineImproving The Livelihoods of Smallholder Fruit Farmers in Soroti District, Teso Sub Region, Eastern Uganda RegionPatricia AngatoNessuna valutazione finora
- Payroll Solution in Single SheetDocumento818 paginePayroll Solution in Single SheetTarique KhanNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Kingdom of AnimaliaDocumento6 pagineKingdom of AnimaliaBen ZerepNessuna valutazione finora
- Tackling Food Inflation: Ashwinkumar Kokku - 67 Malcolm Pinto - 89 Samir Vele - Nitin JadhavDocumento9 pagineTackling Food Inflation: Ashwinkumar Kokku - 67 Malcolm Pinto - 89 Samir Vele - Nitin JadhavMalcolm PintoNessuna valutazione finora
- Glycolysis Krebscycle Practice Questions SCDocumento2 pagineGlycolysis Krebscycle Practice Questions SCapi-323720899Nessuna valutazione finora
- Library PDFDocumento74 pagineLibrary PDFfumiNessuna valutazione finora
- BHP Billiton Petroleum Contract Letter For ABDUL SATTARDocumento5 pagineBHP Billiton Petroleum Contract Letter For ABDUL SATTARAbdul SattarNessuna valutazione finora
- Catalogue CV. Traka Abadi UniversalDocumento15 pagineCatalogue CV. Traka Abadi UniversalHackers StevenNessuna valutazione finora
- Gay Costa Del Sol - 2010Documento2 pagineGay Costa Del Sol - 2010gayinfospainNessuna valutazione finora
- New Book "101 Costly HR Mistakes... and How To Fix Them" by Vanessa Nelson Released To Help Employers Avoid Costly HR Mistakes and Save MillionsDocumento2 pagineNew Book "101 Costly HR Mistakes... and How To Fix Them" by Vanessa Nelson Released To Help Employers Avoid Costly HR Mistakes and Save MillionsPR.comNessuna valutazione finora
- Safety Tips in Playing ArnisDocumento2 pagineSafety Tips in Playing ArnisDensyo De MensyoNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)