Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- PP-PNP-IND-0531 - Evidence Based Decision Choosing PCVDocumento45 paginePP-PNP-IND-0531 - Evidence Based Decision Choosing PCVRohit BharadwajNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Complex Febrile Seizures - Dr. Albert JamesDocumento4 pagineComplex Febrile Seizures - Dr. Albert JamesRohit BharadwajNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- PA-HCP-Role of Nutrition in Surgical PICUDocumento43 paginePA-HCP-Role of Nutrition in Surgical PICURohit BharadwajNessuna valutazione finora
- NUPhD - Protocol - SampleDocumento8 pagineNUPhD - Protocol - SampleRohit BharadwajNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Medicall Private Practice Final PDFDocumento109 pagineMedicall Private Practice Final PDFRohit BharadwajNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Japanese Encephalitis - CME - Slides - Nov - 2020Documento43 pagineJapanese Encephalitis - CME - Slides - Nov - 2020Rohit BharadwajNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Hematenics Vitamins How To ChooseDocumento27 pagineHematenics Vitamins How To ChooseRohit BharadwajNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Picky Eaters vs. Feeding Disorders: Recognizing The DifferencesDocumento33 paginePicky Eaters vs. Feeding Disorders: Recognizing The DifferencesRohit BharadwajNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 947 Newly Diagnosed Diabetic ChildDocumento16 pagine947 Newly Diagnosed Diabetic ChildRohit BharadwajNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Types of LRs - Sheet2Documento2 pagineTypes of LRs - Sheet2Rohit BharadwajNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Bristol Pain DocumentDocumento79 pagineBristol Pain DocumentRohit BharadwajNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Comprehensive Review of Meningococcal Disease Burden in IndiaDocumento23 pagineA Comprehensive Review of Meningococcal Disease Burden in IndiaRohit BharadwajNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Choosing A Right Probiotic in Acute GE in Children 2022 - 11apr22 - VFDocumento38 pagineChoosing A Right Probiotic in Acute GE in Children 2022 - 11apr22 - VFRohit BharadwajNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Amp Designer Cheat SheetDocumento26 pagineAmp Designer Cheat SheetRohit BharadwajNessuna valutazione finora
- MEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Documento4 pagineMEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Rohit BharadwajNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- VWD June 2019Documento5 pagineVWD June 2019Rohit BharadwajNessuna valutazione finora
- Self-Assessment: QuestionsDocumento4 pagineSelf-Assessment: QuestionsRohit BharadwajNessuna valutazione finora
- Diagnosis and Management of Pediatric Autoimmune PDFDocumento16 pagineDiagnosis and Management of Pediatric Autoimmune PDFRamina PasariNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Lecture 4 Questions & AnswersDocumento6 pagineLecture 4 Questions & AnswersRohit BharadwajNessuna valutazione finora
- Boho Beautiful: Class ListDocumento4 pagineBoho Beautiful: Class ListRohit BharadwajNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- NephrologyDocumento9 pagineNephrologyRohit BharadwajNessuna valutazione finora
- PHE Meningo Disease GuidelineDocumento54 paginePHE Meningo Disease GuidelineRohit BharadwajNessuna valutazione finora
- pGALs Screening Questions 6965Documento2 paginepGALs Screening Questions 6965Rohit BharadwajNessuna valutazione finora
- The 17th Expert Consensus Document of The European Bifurcation Club Techniques TDocumento11 pagineThe 17th Expert Consensus Document of The European Bifurcation Club Techniques TValentin CHIONCELNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Module 13 - Cystoclysis (Student)Documento4 pagineModule 13 - Cystoclysis (Student)Raymond Edge100% (2)
- Crash Cart Check ListDocumento2 pagineCrash Cart Check ListMenGuitarNessuna valutazione finora
- Lap Juli 2019Documento144 pagineLap Juli 2019Asrina Ambo RakkaNessuna valutazione finora
- Schedule D: List of Life Saveing or Life Sustaining Medical DevicesDocumento5 pagineSchedule D: List of Life Saveing or Life Sustaining Medical DevicesAasma RehmanNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- CRASH CART ArrangementDocumento2 pagineCRASH CART Arrangementsabbo mors0% (1)
- Urinary Catheterization: By: Michael John Z. Principio, RN, RM, MancDocumento22 pagineUrinary Catheterization: By: Michael John Z. Principio, RN, RM, MancSarahlaine BrazasNessuna valutazione finora
- 2016-Brochure Umbilical CatheterDocumento4 pagine2016-Brochure Umbilical CatheterSuman MondalNessuna valutazione finora
- Description:: Materials/ Equipment NeededDocumento6 pagineDescription:: Materials/ Equipment NeededMarc Renz R. ChanNessuna valutazione finora
- Removing Indwelling CatheterDocumento1 paginaRemoving Indwelling CatheterAngelie PantajoNessuna valutazione finora
- Catherization Insertion and Removal of An Indwelling Catheter DateDocumento2 pagineCatherization Insertion and Removal of An Indwelling Catheter DatecarlyNessuna valutazione finora
- Urinary CatheterizationDocumento11 pagineUrinary CatheterizationPamDavidGabrielNessuna valutazione finora
- Misamis University: CatheterizationDocumento6 pagineMisamis University: CatheterizationNiña Jean Tormis AldabaNessuna valutazione finora
- Urine Procedure WordDocumento27 pagineUrine Procedure WordYashly VargheseNessuna valutazione finora
- Crash Cart Policy and Checklist in Hospital TraningDocumento4 pagineCrash Cart Policy and Checklist in Hospital TraningPRADIPNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
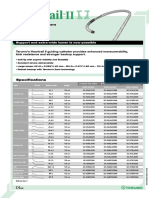
- PTCA Guiding Catheters: SpecificationsDocumento6 paginePTCA Guiding Catheters: Specificationsricardo paulettoNessuna valutazione finora
- Hemant Surgical Double Lumen CathetersDocumento2 pagineHemant Surgical Double Lumen CathetersKaushik Hanskumar ShahNessuna valutazione finora
- Demo 2Documento6 pagineDemo 2Justine VillaflorNessuna valutazione finora
- QI - Patient Safety Project Plan Presentation - Storyboard TemplateDocumento1 paginaQI - Patient Safety Project Plan Presentation - Storyboard TemplateoliviajuolaNessuna valutazione finora
- Cardiac Catheterization and Coronary AngiographyDocumento5 pagineCardiac Catheterization and Coronary Angiographyedem100% (1)
- 10 Oropharyngeal and Nasopharyngeal SuctioningDocumento8 pagine10 Oropharyngeal and Nasopharyngeal SuctioningKen Morales Alcantara100% (1)
- PGH 101 v2018Documento10 paginePGH 101 v2018Ian Phillip PaclibareNessuna valutazione finora
- SKILL: Oropharyngeal and Nasopharyngeal SuctioningDocumento3 pagineSKILL: Oropharyngeal and Nasopharyngeal SuctioningCherry Rose Arce SamsonNessuna valutazione finora
- Bladder Irrigation (Cystoclysis)Documento4 pagineBladder Irrigation (Cystoclysis)CJ Angeles100% (2)
- First Aid Bandaging & Splinting Simulator SpecificationsDocumento7 pagineFirst Aid Bandaging & Splinting Simulator SpecificationsNyucel WellnessNessuna valutazione finora
- Colostomy Care - ChecklistDocumento6 pagineColostomy Care - Checklistcriszangot71% (7)
- Urinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Documento9 pagineUrinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Franz goNessuna valutazione finora
- 672 - Trial Without Catheter - TWOCDocumento8 pagine672 - Trial Without Catheter - TWOCTanaman PeternakanNessuna valutazione finora
- Angiography PreparationsDocumento14 pagineAngiography PreparationsAndrei BulgariuNessuna valutazione finora
- Tubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterDocumento11 pagineTubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterJeremy HamptonNessuna valutazione finora