Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- ENFERMERÍA EN CUIDADOS PALIATIVOS Tomo I - Eulalia López ImedioDocumento207 pagineENFERMERÍA EN CUIDADOS PALIATIVOS Tomo I - Eulalia López ImedioodlgalindoNessuna valutazione finora
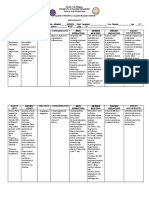
- Spina Bifida Concept Map PDFDocumento1 paginaSpina Bifida Concept Map PDFnot realNessuna valutazione finora
- Simulación - Clínica e Investigación en Pre-HospitalarioDocumento6 pagineSimulación - Clínica e Investigación en Pre-HospitalarioodlgalindoNessuna valutazione finora
- Comparison of Continuous Thermodilution and Bolus CO MeasureDocumento5 pagineComparison of Continuous Thermodilution and Bolus CO MeasureodlgalindoNessuna valutazione finora
- Tracheal Intubation Practice and Safety Across International PICUs A Report From National Emergency Airway Registry For ChildrenDocumento8 pagineTracheal Intubation Practice and Safety Across International PICUs A Report From National Emergency Airway Registry For ChildrenodlgalindoNessuna valutazione finora
- CaredeliverymodelDocumento9 pagineCaredeliverymodelodlgalindoNessuna valutazione finora
- CaredeliverymodelDocumento9 pagineCaredeliverymodelodlgalindoNessuna valutazione finora
- Educación Basada en Simulación-Debriefing Sus Bondades y DificultadesDocumento10 pagineEducación Basada en Simulación-Debriefing Sus Bondades y DificultadesodlgalindoNessuna valutazione finora
- CaredeliverymodelDocumento9 pagineCaredeliverymodelodlgalindoNessuna valutazione finora
- AhsokaDocumento164 pagineAhsokaodlgalindo100% (1)
- DV Sos #5 PDFDocumento24 pagineDV Sos #5 PDFodlgalindoNessuna valutazione finora
- 09 - Darth Vader Lord of The Sith #4Documento23 pagine09 - Darth Vader Lord of The Sith #4odlgalindoNessuna valutazione finora
- DV Sos #6Documento24 pagineDV Sos #6odlgalindoNessuna valutazione finora
- 09 - Darth Vader Lord of The Sith #3Documento24 pagine09 - Darth Vader Lord of The Sith #3odlgalindoNessuna valutazione finora
- Darth Maul 5Documento23 pagineDarth Maul 5odlgalindoNessuna valutazione finora
- Darth Maul 4Documento22 pagineDarth Maul 4odlgalindoNessuna valutazione finora
- Darth Maul 1Documento33 pagineDarth Maul 1odlgalindoNessuna valutazione finora
- Darth Maul 2Documento23 pagineDarth Maul 2odlgalindoNessuna valutazione finora
- Darth Maul 3Documento23 pagineDarth Maul 3odlgalindoNessuna valutazione finora
- Star Wars 26Documento22 pagineStar Wars 26odlgalindoNessuna valutazione finora
- Intro To Aseptic DispensingDocumento64 pagineIntro To Aseptic DispensingGhan Longo Leng100% (1)
- 2A - Pasay - Module 3 - Explain PharmacologyDocumento6 pagine2A - Pasay - Module 3 - Explain PharmacologyTrishaNessuna valutazione finora
- Gastroretentive Drug Delivery System A ReviewDocumento10 pagineGastroretentive Drug Delivery System A ReviewEditor IJTSRDNessuna valutazione finora
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Documento3 pagineHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNessuna valutazione finora
- MCQ - Discussion On DM: DR Aditi Chaturvedi Prof. and Head Department of PharmacologyDocumento57 pagineMCQ - Discussion On DM: DR Aditi Chaturvedi Prof. and Head Department of PharmacologyVijay SharmaNessuna valutazione finora
- OxybutyninDocumento2 pagineOxybutynin3S - JOCSON, DENESE NICOLE LEE M.Nessuna valutazione finora
- 8 Propofol Drug StudyDocumento4 pagine8 Propofol Drug Studyshadow gonzalez100% (1)
- Drug Study (Aspirin)Documento3 pagineDrug Study (Aspirin)Mae Therese B. MAGNONessuna valutazione finora
- 5 Anti - Inflammatory Drugs, Anti-Gout DrugsDocumento15 pagine5 Anti - Inflammatory Drugs, Anti-Gout DrugsAudrey Beatrice ReyesNessuna valutazione finora
- D. Barlow - Cognitive-Behavioral Treatment For Panic Disorder Current StatusDocumento16 pagineD. Barlow - Cognitive-Behavioral Treatment For Panic Disorder Current StatusArmando ValladaresNessuna valutazione finora
- Diabetes Type 2 Treatment AlgorithmDocumento25 pagineDiabetes Type 2 Treatment AlgorithmJ Wong100% (1)
- Metoclopramide Drug StudyDocumento2 pagineMetoclopramide Drug StudyRem remNessuna valutazione finora
- Prescribed Medication: Information Leaflet PriorDocumento4 paginePrescribed Medication: Information Leaflet PriorHavier EsparagueraNessuna valutazione finora
- Sr. No. Product Name Packing-All Are Alu-Pvc Blisterfor Tab Cap - For Syrup Pet BottleDocumento2 pagineSr. No. Product Name Packing-All Are Alu-Pvc Blisterfor Tab Cap - For Syrup Pet Bottlesanjay_gawaliNessuna valutazione finora
- Tourette'S Disorder: Presented byDocumento14 pagineTourette'S Disorder: Presented byjaydipNessuna valutazione finora
- Lesson 18 - Pricelist of MedicinesDocumento4 pagineLesson 18 - Pricelist of MedicinesGrace RepolloNessuna valutazione finora
- Polymers in Drug Delivery Technology, Types of Polymers and ApplicationsDocumento4 paginePolymers in Drug Delivery Technology, Types of Polymers and ApplicationsSharanya ParamshettiNessuna valutazione finora
- Topoisomerases Structure Function and MechanismDocumento15 pagineTopoisomerases Structure Function and MechanismAnkeet KumarNessuna valutazione finora
- AllergyDocumento23 pagineAllergyAmbl GeronNessuna valutazione finora
- List-European-Union-Reference-Dates-Frequency-Submission-Periodic-Safety-Update-Reports - en (2) UpdatedDocumento40 pagineList-European-Union-Reference-Dates-Frequency-Submission-Periodic-Safety-Update-Reports - en (2) UpdatedMai MostafaNessuna valutazione finora
- Pleural EffusionDocumento78 paginePleural EffusionJessa AdenigNessuna valutazione finora
- Sotalol Drug CardDocumento2 pagineSotalol Drug CardJanet SheldonNessuna valutazione finora
- Literature Review PharmacyDocumento4 pagineLiterature Review Pharmacyafdtlgezo100% (1)
- Nutraceuticals: Assignment 1Documento10 pagineNutraceuticals: Assignment 1Nguyễn DungNessuna valutazione finora
- Annex I Summary of Product CharacteristicsDocumento34 pagineAnnex I Summary of Product CharacteristicsLaura RačytėNessuna valutazione finora
- Asthma Management and Prevention in ChildrenDocumento57 pagineAsthma Management and Prevention in ChildrenSundararajaperumal AnandhakrishnanNessuna valutazione finora
- ICU Cheat SheetDocumento2 pagineICU Cheat SheetPrescilla Randazzo100% (1)
- Welcome To Course Title: Clinical Pharmacy Topic: TDM of DigoxinDocumento16 pagineWelcome To Course Title: Clinical Pharmacy Topic: TDM of DigoxinUmair MazharNessuna valutazione finora
- Antacid Drug AnalysisDocumento2 pagineAntacid Drug AnalysisJosef Angelo PoldoNessuna valutazione finora