Potrebbero piacerti anche
- PQCNC NHPC LS3 Devente 20200310Documento8 paginePQCNC NHPC LS3 Devente 20200310kcochranNessuna valutazione finora
- PQCNC Kickoff Meeting Agenda 2019Documento1 paginaPQCNC Kickoff Meeting Agenda 2019kcochranNessuna valutazione finora
- Preterm+Prelabour+Rupture+of+the+Membranes Sept2015Documento12 paginePreterm+Prelabour+Rupture+of+the+Membranes Sept2015molenNessuna valutazione finora
- GA by Ultrasound SOGCDocumento11 pagineGA by Ultrasound SOGCBrendaNessuna valutazione finora
- Clinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineDocumento10 pagineClinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineUtomo BudidarmoNessuna valutazione finora
- Hyperinsulinisminthe Neonate: Katherine Lord,, Diva D. de LeónDocumento14 pagineHyperinsulinisminthe Neonate: Katherine Lord,, Diva D. de LeónMaría Paula Sarmiento RamónNessuna valutazione finora
- Paracetamol in NeonatusDocumento7 pagineParacetamol in Neonatusnurul sya'binNessuna valutazione finora
- Prune Belly SyndromeDocumento46 paginePrune Belly SyndromebadbearpstNessuna valutazione finora
- NEC Societys Probiotics Statement - ShareDocumento3 pagineNEC Societys Probiotics Statement - Shareendy tovarNessuna valutazione finora
- Friedman VTE Bundle PDFDocumento24 pagineFriedman VTE Bundle PDFGerman Parra CNessuna valutazione finora
- Blood - BLD 2022 016558 C MainDocumento12 pagineBlood - BLD 2022 016558 C MaincnshematologiaNessuna valutazione finora
- Cuidados Del Egresado de UCINDocumento20 pagineCuidados Del Egresado de UCINIsabel Soto ANessuna valutazione finora
- Double Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF:ICSI Programmes (Shanghai Protocol) - ScienceDirectDocumento3 pagineDouble Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF:ICSI Programmes (Shanghai Protocol) - ScienceDirectsamirNessuna valutazione finora
- Platelet Transfusion 2021Documento14 paginePlatelet Transfusion 2021Raymond RosarioNessuna valutazione finora
- Perdarahan Postpartum PIT IDI Bekasi 2016Documento44 paginePerdarahan Postpartum PIT IDI Bekasi 2016Julia AstriNessuna valutazione finora
- En - Practical Approach.2010Documento13 pagineEn - Practical Approach.2010rendyjiwonoNessuna valutazione finora
- DR Poli Obs Ii Mug 01.03.19Documento22 pagineDR Poli Obs Ii Mug 01.03.19mughanNessuna valutazione finora
- Approach To Cyanosis in A NeonateDocumento8 pagineApproach To Cyanosis in A NeonateSujeetNessuna valutazione finora
- Motherisk Update: Is Air Travel in Pregnancy Safe?Documento2 pagineMotherisk Update: Is Air Travel in Pregnancy Safe?triNessuna valutazione finora
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDocumento38 paginePtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- VICTORIA, Cesar - Breastfeeding in The 21st Century - The Lancet PDFDocumento39 pagineVICTORIA, Cesar - Breastfeeding in The 21st Century - The Lancet PDFJorge López GagoNessuna valutazione finora
- Urinary Tract Infection in Children Diagnosis, Treatment, Imaging - Comparison of Current Guidelines 10.1016@j.jpurol.2017.07.018Documento7 pagineUrinary Tract Infection in Children Diagnosis, Treatment, Imaging - Comparison of Current Guidelines 10.1016@j.jpurol.2017.07.018Gyanendra SharmaNessuna valutazione finora
- Cerebroplacental Ratio in Fetal Well Being Assessment in SGA and AGA FetusDocumento11 pagineCerebroplacental Ratio in Fetal Well Being Assessment in SGA and AGA FetuspolygoneNessuna valutazione finora
- Journal Pmed 1003787Documento20 pagineJournal Pmed 1003787GAYATHIRINessuna valutazione finora
- Contraceptivemethods 150521003728 Lva1 App6892Documento59 pagineContraceptivemethods 150521003728 Lva1 App6892Michael John Anicas LozanoNessuna valutazione finora
- Rational Antibiotic Practice: Under IAP Action Plan 2014 Academic Grant From Delcure PharmaDocumento164 pagineRational Antibiotic Practice: Under IAP Action Plan 2014 Academic Grant From Delcure PharmaGurmeet SinghNessuna valutazione finora
- Panduan Feeding IndiaDocumento41 paginePanduan Feeding IndiaannisatrieNessuna valutazione finora
- Gina Pocket 2009 Pediatrico Unlocked)Documento21 pagineGina Pocket 2009 Pediatrico Unlocked)Anonymous L9qkHGXNessuna valutazione finora
- Neoreviews: Moc MocDocumento76 pagineNeoreviews: Moc Mocsalamred100% (2)
- Neonatalseizureclinicalguideline PDFDocumento15 pagineNeonatalseizureclinicalguideline PDFNURUL NADIA BINTI MOHD NAZIR / UPMNessuna valutazione finora
- Kompre SemuaDocumento142 pagineKompre SemuaRatna SetiawatiNessuna valutazione finora
- Myop in PregnancyDocumento4 pagineMyop in PregnancySamuel WilliamsNessuna valutazione finora
- 05.endocrine System 4 Blocks PDFDocumento790 pagine05.endocrine System 4 Blocks PDFNicolás LaverdeNessuna valutazione finora
- Feeding The Preterm-ConsensusDocumento124 pagineFeeding The Preterm-ConsensusJuan Diego Lázaro TorresNessuna valutazione finora
- Abstract Scientific Program BookDocumento158 pagineAbstract Scientific Program BookMukand PathakNessuna valutazione finora
- Leptospirosis National Guidelines - Sri LankaDocumento56 pagineLeptospirosis National Guidelines - Sri LankaBrainy-Paykiesaurus LuminirexNessuna valutazione finora
- Acog Committee Opinion: Air Travel During PregnancyDocumento3 pagineAcog Committee Opinion: Air Travel During PregnancyHermus Espiritu Maturrano100% (1)
- PQCNC 2023 Implementing Cardiac Bundle in NCDocumento33 paginePQCNC 2023 Implementing Cardiac Bundle in NCkcochranNessuna valutazione finora
- Maternal Recognition of Pregnancy in Domestic AnimalsDocumento3 pagineMaternal Recognition of Pregnancy in Domestic AnimalsAjay YadavNessuna valutazione finora
- Lactation InsufficiencyDocumento10 pagineLactation InsufficiencyThomas Regina PutraNessuna valutazione finora
- 1st & 2nd Trimester Pregnancy LossDocumento48 pagine1st & 2nd Trimester Pregnancy LossAbdullah EssaNessuna valutazione finora
- SKP DR - IinDocumento57 pagineSKP DR - IinzeniNessuna valutazione finora
- Night Shift Duty Friday, May 15 2020Documento3 pagineNight Shift Duty Friday, May 15 2020Dave OrlandoNessuna valutazione finora
- Case Report: Bayangkara Hospital September 3th-6th 2017 Nurkamilawati AristaDocumento10 pagineCase Report: Bayangkara Hospital September 3th-6th 2017 Nurkamilawati AristanurkamilawatiNessuna valutazione finora
- HIVDocumento299 pagineHIVJhonrie PakiwagNessuna valutazione finora
- Orar Mo 4 Sem1 2021 2022 VF S6 14Documento26 pagineOrar Mo 4 Sem1 2021 2022 VF S6 14Vasiliu LăcrămioaraNessuna valutazione finora
- CR3 RobbbDocumento86 pagineCR3 RobbbIhsan Rasyid YuldiNessuna valutazione finora
- RMS Senior B SumbawaDocumento11 pagineRMS Senior B Sumbawaimamsantos1191Nessuna valutazione finora
- Master Teachers DevelopmentDocumento3 pagineMaster Teachers Developmentαλβιν δεNessuna valutazione finora
- CHARTSDocumento14 pagineCHARTSR ArcegaNessuna valutazione finora
- ENDORSEMENT SX DraftDocumento3 pagineENDORSEMENT SX DraftRED STATIONNessuna valutazione finora
- Foundation of Our Lady of Peace Mission, IncDocumento6 pagineFoundation of Our Lady of Peace Mission, IncER MorsalinNessuna valutazione finora
- Mo2 OrarS2 20 v3 PDFDocumento2 pagineMo2 OrarS2 20 v3 PDFMitchell CarterNessuna valutazione finora
- HU 01 IC 2023-1 02-C3 2022-321225 RegAux Consolido-2Documento2 pagineHU 01 IC 2023-1 02-C3 2022-321225 RegAux Consolido-2Juan Antenor Caceda CorillocllaNessuna valutazione finora
- CR Poli Obs 11-05-18 EditDocumento133 pagineCR Poli Obs 11-05-18 EditRyan IlhamNessuna valutazione finora
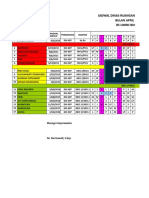
- Jadwal Perinatologi April 2019Documento2 pagineJadwal Perinatologi April 2019Muhamad NidanNessuna valutazione finora
- Daftar Dinas Pegawai Rsu. Bunda Thamrin Ruangan Ok Bulan: Januari 2021Documento30 pagineDaftar Dinas Pegawai Rsu. Bunda Thamrin Ruangan Ok Bulan: Januari 2021Sulastri PasaribuNessuna valutazione finora
- Orar RI An III Sem II 2022-2023Documento5 pagineOrar RI An III Sem II 2022-2023Bogdan ArdeleanNessuna valutazione finora
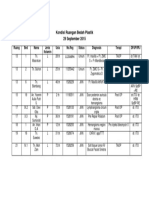
- Konru Bedah Plastik 29 September 2015Documento1 paginaKonru Bedah Plastik 29 September 2015mariskaNessuna valutazione finora
- 13/7/2021 Tuesday: RN: Wu Chu NxiangDocumento5 pagine13/7/2021 Tuesday: RN: Wu Chu NxiangHadzrie HamdanNessuna valutazione finora
- PQCNC 2024 Kickoff Long Story Short 20240110Documento26 paginePQCNC 2024 Kickoff Long Story Short 20240110kcochranNessuna valutazione finora
- PQCNC 2024 Initiative - Maternal SepsisDocumento12 paginePQCNC 2024 Initiative - Maternal SepsiskcochranNessuna valutazione finora
- PQCNC 2024 Kickoff OB Sepsis Statewide Implementation 20240116Documento33 paginePQCNC 2024 Kickoff OB Sepsis Statewide Implementation 20240116kcochranNessuna valutazione finora
- PQCNC clOUDi LS2 OUD Pregnancy RyanDocumento53 paginePQCNC clOUDi LS2 OUD Pregnancy RyankcochranNessuna valutazione finora
- PQCNC 2024 Initiative Maternal CardiacDocumento30 paginePQCNC 2024 Initiative Maternal CardiackcochranNessuna valutazione finora
- PQCNC 2023 Supporting The Diagnosis and Treatment of Severe HTNDocumento11 paginePQCNC 2023 Supporting The Diagnosis and Treatment of Severe HTNkcochranNessuna valutazione finora
- PQCNC 2023 Implementing Cardiac Bundle in NCDocumento33 paginePQCNC 2023 Implementing Cardiac Bundle in NCkcochranNessuna valutazione finora
- PQCNC 2023 Nutrition in PregnancyDocumento12 paginePQCNC 2023 Nutrition in PregnancykcochranNessuna valutazione finora
- PQCNC 2023 Standardizing The Care of Late-Preterm InfantsDocumento17 paginePQCNC 2023 Standardizing The Care of Late-Preterm InfantskcochranNessuna valutazione finora
- PQCNC clOUDi LS2 SUD Trauma PregnancyDocumento31 paginePQCNC clOUDi LS2 SUD Trauma PregnancykcochranNessuna valutazione finora
- PQCNC 2023 ClOUDi Continuation 2.0Documento12 paginePQCNC 2023 ClOUDi Continuation 2.0kcochranNessuna valutazione finora
- PQCNC 2023 Safe SleepDocumento13 paginePQCNC 2023 Safe SleepkcochranNessuna valutazione finora
- PQCNC AIM RPC LS2 Volunteer Doula ProgramDocumento23 paginePQCNC AIM RPC LS2 Volunteer Doula ProgramkcochranNessuna valutazione finora
- PQCNC NHPC LS3 Noel 2020 Workload Indicators 20200310.Documento23 paginePQCNC NHPC LS3 Noel 2020 Workload Indicators 20200310.kcochranNessuna valutazione finora
- PQCNC 2023 Enhancing Perinatal Mental HealthDocumento10 paginePQCNC 2023 Enhancing Perinatal Mental HealthkcochranNessuna valutazione finora
- PQCNC 2023 Improving The Use of Mother's Milk at DischargeDocumento8 paginePQCNC 2023 Improving The Use of Mother's Milk at DischargekcochranNessuna valutazione finora
- PQCNC clOUDi Kickoff Main 2021Documento27 paginePQCNC clOUDi Kickoff Main 2021kcochranNessuna valutazione finora
- North Carolina Perinatal Quality Collaborative Initiative: Standardizing Perinatal Substance Use ScreeningDocumento41 pagineNorth Carolina Perinatal Quality Collaborative Initiative: Standardizing Perinatal Substance Use ScreeningkcochranNessuna valutazione finora
- PQCNC clOUDi Kickoff Data 2021Documento13 paginePQCNC clOUDi Kickoff Data 2021kcochranNessuna valutazione finora
- PQCNC NHPC LS3 Vidant Panel 20200310Documento4 paginePQCNC NHPC LS3 Vidant Panel 20200310kcochranNessuna valutazione finora
- PQCNC NHPC LS3 Mccaffrey 20200310Documento29 paginePQCNC NHPC LS3 Mccaffrey 20200310kcochran100% (1)
- PQCNC AIM RPC LS3 Ketner Posting 20200303Documento41 paginePQCNC AIM RPC LS3 Ketner Posting 20200303kcochranNessuna valutazione finora
- Newborn Hypoglycemia Prevention and CareDocumento30 pagineNewborn Hypoglycemia Prevention and CarekcochranNessuna valutazione finora
- PQCNC AIM RPC LS3 Data 20200303Documento16 paginePQCNC AIM RPC LS3 Data 20200303kcochranNessuna valutazione finora
- PQCNC AIM RPC Spinning BabiesDocumento71 paginePQCNC AIM RPC Spinning Babieskcochran50% (2)
- PQCNC AIM RPC LS2 Scheduling To Improve Labor SupportDocumento20 paginePQCNC AIM RPC LS2 Scheduling To Improve Labor SupportkcochranNessuna valutazione finora
- Novant Health Forsyth Medical Center: Parent Engagement and Integrated CareDocumento13 pagineNovant Health Forsyth Medical Center: Parent Engagement and Integrated CarekcochranNessuna valutazione finora
- IV Fluids in The Mother Baby Unit: Meghan Dougherty, MDDocumento8 pagineIV Fluids in The Mother Baby Unit: Meghan Dougherty, MDkcochranNessuna valutazione finora
- PQCNCNHPCLS2 FINALVidant Scheller 20191014Documento22 paginePQCNCNHPCLS2 FINALVidant Scheller 20191014kcochranNessuna valutazione finora
- NURSING CARE PLAN OcdDocumento25 pagineNURSING CARE PLAN Ocdkiran mahal81% (26)
- MOST Assign1 VitaminsDocumento6 pagineMOST Assign1 VitaminsbubblingbrookNessuna valutazione finora
- As NZS 3824-1998 Guidelines For Radiotherapy Treatment Rooms DesignDocumento10 pagineAs NZS 3824-1998 Guidelines For Radiotherapy Treatment Rooms DesignSAI Global - APACNessuna valutazione finora
- Hyperthermia in Cancer Treatment: Cabuy E. Reliable Cancer Therapies. Energy-Based Therapies. 2011 1 (2) :1-48Documento48 pagineHyperthermia in Cancer Treatment: Cabuy E. Reliable Cancer Therapies. Energy-Based Therapies. 2011 1 (2) :1-48Eliza LlenzaNessuna valutazione finora
- Biochemistry LaboratoryDocumento6 pagineBiochemistry LaboratoryMark Benedict MontalboNessuna valutazione finora
- MEDSDocumento4 pagineMEDSMegan DirigeNessuna valutazione finora
- Adrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenDocumento33 pagineAdrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenHendra EfendiNessuna valutazione finora
- Analysis Journal ContentsDocumento10 pagineAnalysis Journal ContentsSLNessuna valutazione finora
- Prevention of Crown and Root Caries in AdultsDocumento19 paginePrevention of Crown and Root Caries in AdultsnataliaNessuna valutazione finora
- Standard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCDocumento4 pagineStandard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCJaijeev PaliNessuna valutazione finora
- Analysis of Synthetic CannabinoidsDocumento13 pagineAnalysis of Synthetic CannabinoidsLuděk SpurnýNessuna valutazione finora
- Introduction To Statistical MethodsDocumento197 pagineIntroduction To Statistical Methodsulastuna2001100% (1)
- Drug Screening Questionnaire DASTDocumento2 pagineDrug Screening Questionnaire DASTErin CooperNessuna valutazione finora
- Tugas Bahasa InggrisDocumento14 pagineTugas Bahasa InggrisAlfin MT16Nessuna valutazione finora
- Letter of RecomendationDocumento2 pagineLetter of RecomendationJorge Luis Sánchez Alarcón100% (1)
- Psychiatric Nursing Mastery Test Part 2Documento16 paginePsychiatric Nursing Mastery Test Part 2Rika MaeNessuna valutazione finora
- 04 21 HealthDocumento16 pagine04 21 HealthMoga RazvanNessuna valutazione finora
- INTENSIVE CARE UNIT Gurugram Civil HospitalDocumento7 pagineINTENSIVE CARE UNIT Gurugram Civil HospitalOmprakash Sundrani100% (1)
- Dengue (Break Bone Fever) - FAQ, DPH-TAMIL NADU, IndiaDocumento3 pagineDengue (Break Bone Fever) - FAQ, DPH-TAMIL NADU, IndiaDr.SagindarNessuna valutazione finora
- Prof. Rajnish Wattas ArticleDocumento8 pagineProf. Rajnish Wattas ArticleSurya EduNessuna valutazione finora
- Varicose VeinDocumento22 pagineVaricose VeinKamalNessuna valutazione finora
- The Fitness Project 2018Documento34 pagineThe Fitness Project 2018San joe50% (2)
- ATI DRUG TABLES Module4 Respiratory Glucocorticoids InhalationDocumento1 paginaATI DRUG TABLES Module4 Respiratory Glucocorticoids InhalationnoeyeshaveseenNessuna valutazione finora
- Palaska 2014Documento10 paginePalaska 2014Marco TeixeiraNessuna valutazione finora
- Mental Health ServicesDocumento6 pagineMental Health Servicesapi-494539289Nessuna valutazione finora
- Lung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Documento53 pagineLung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Mr. IncognitoNessuna valutazione finora
- Acog Practice Bulletin Summary: Management of Symptomatic Uterine LeiomyomasDocumento3 pagineAcog Practice Bulletin Summary: Management of Symptomatic Uterine LeiomyomasMariana Hernandez100% (6)
- Glucose-Loesung 5 08-07 03Documento2 pagineGlucose-Loesung 5 08-07 03Andreea CaticiNessuna valutazione finora
- Tammy, 2011. Drug Interaction PDFDocumento14 pagineTammy, 2011. Drug Interaction PDFdyahNessuna valutazione finora
- Classification of Bone Tumors NewDocumento38 pagineClassification of Bone Tumors NewSyed WahajNessuna valutazione finora