Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Rmdjv-pj74-Hiradc-subc 03 (Hoisting & Rigging)Documento1 paginaRmdjv-pj74-Hiradc-subc 03 (Hoisting & Rigging)myn maliQueNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Vital Spots 10 - Taranaki ITF Taekwondo PDFDocumento54 pagineVital Spots 10 - Taranaki ITF Taekwondo PDFMaria Elisa MonclusNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Surface Anatomy: de La Salle-Lipa College of LawDocumento79 pagineSurface Anatomy: de La Salle-Lipa College of LawFatzie MendozaNessuna valutazione finora
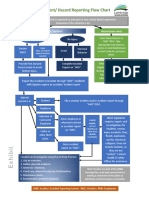
- Accident Incident Reporting FlowchartDocumento1 paginaAccident Incident Reporting Flowchartsyamimi balkhisNessuna valutazione finora
- Iyengar Yoga UK SyllabusDocumento13 pagineIyengar Yoga UK SyllabusSummit Gautam100% (1)
- Principles of Malunion ManagementDocumento51 paginePrinciples of Malunion Managementdioz100% (1)
- Principles of MRPDocumento24 paginePrinciples of MRPShriya100% (1)
- PERCEPTION-COORDINATION-PRE-TEST RationalizationDocumento11 paginePERCEPTION-COORDINATION-PRE-TEST Rationalizationdrei yanNessuna valutazione finora
- Extensor Apparatus of The Lesser Toes - Anatomy With Clinical Implications-Topical Review - Foot and Ankle Int PDFDocumento14 pagineExtensor Apparatus of The Lesser Toes - Anatomy With Clinical Implications-Topical Review - Foot and Ankle Int PDFHeliosNessuna valutazione finora
- Tendon Transfers - Paralytic DeformityDocumento19 pagineTendon Transfers - Paralytic DeformityHeliosNessuna valutazione finora
- Section SL11Documento6 pagineSection SL11KostYurNessuna valutazione finora
- Angiosomes 1Documento33 pagineAngiosomes 1HeliosNessuna valutazione finora
- Phases of The PushupDocumento2 paginePhases of The PushupMaryane AngelaNessuna valutazione finora
- Genereal Examination-Anukul SurgeryDocumento4 pagineGenereal Examination-Anukul SurgeryTRASH MAILNessuna valutazione finora
- FHP ResearchDocumento61 pagineFHP ResearchPooja DaveNessuna valutazione finora
- Hip Fracture Programme: A Guide For Patients Following SurgeryDocumento20 pagineHip Fracture Programme: A Guide For Patients Following SurgeryDruga DanutNessuna valutazione finora
- Briggs and Straton Operators Manual 1Documento136 pagineBriggs and Straton Operators Manual 1Robert DelafosseNessuna valutazione finora
- SSO Shoulder SLAP Surgery RehabilitationDocumento10 pagineSSO Shoulder SLAP Surgery RehabilitationDruga DanutNessuna valutazione finora
- Case Presentation OrifDocumento27 pagineCase Presentation OrifANJELO CYRUS BIARES GARCIANessuna valutazione finora
- Consenso LCL Chahla2018Documento10 pagineConsenso LCL Chahla2018Nuno AlimanNessuna valutazione finora
- Infograph Regarding Dance Related FitnessDocumento2 pagineInfograph Regarding Dance Related FitnessMendoza PeeviNessuna valutazione finora
- Forces During Squatting and Rising From A Deep Squat: SeedhomDocumento8 pagineForces During Squatting and Rising From A Deep Squat: SeedhomAnsar LawiNessuna valutazione finora
- October 30, 2020 Joanna DurkanDocumento2 pagineOctober 30, 2020 Joanna DurkanMihai Alexandru TomaNessuna valutazione finora
- Quintanaetal 2011NURALAGUSREXGEN ETSP NOV ANENDEMICINSULARGIANTRABBITFROMTHENEOGENEOFMINORCABALEARICISLANDSSPAINDocumento11 pagineQuintanaetal 2011NURALAGUSREXGEN ETSP NOV ANENDEMICINSULARGIANTRABBITFROMTHENEOGENEOFMINORCABALEARICISLANDSSPAINErick Javier Calderon MoralesNessuna valutazione finora
- Libble EuDocumento32 pagineLibble EuIvan AzenicNessuna valutazione finora
- Titanium Plates and Screws For Open Wedge HtoDocumento6 pagineTitanium Plates and Screws For Open Wedge HtoDaniel Quijada LucarioNessuna valutazione finora
- DodgeballDocumento5 pagineDodgeballapi-514548596Nessuna valutazione finora
- Proper Techniques for Transporting Injured VictimsDocumento4 pagineProper Techniques for Transporting Injured VictimsJazzy Anne AquinoNessuna valutazione finora
- Anaerobic BacteriaDocumento4 pagineAnaerobic BacteriaJesette KhoNessuna valutazione finora
- Bone Fracture Types, Causes, Signs and TreatmentDocumento23 pagineBone Fracture Types, Causes, Signs and TreatmentGizachew AsimareNessuna valutazione finora
- Near Miss Reporting: A Tool for SafetyDocumento2 pagineNear Miss Reporting: A Tool for Safetypruncu.alianmNessuna valutazione finora
- Staircase and Walkways Railing Work JSA HSE ProfessionalsDocumento1 paginaStaircase and Walkways Railing Work JSA HSE ProfessionalsSamadov 13Nessuna valutazione finora
- Esophageal cancer causes miseryDocumento21 pagineEsophageal cancer causes miseryHuram SeremaniNessuna valutazione finora
- Oral RecitationDocumento1 paginaOral RecitationRyan AntonioNessuna valutazione finora