Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- DMSO Benefits and Uses-Also Send MMS+LiverBal+Quinine - 2.25.21Documento6 pagineDMSO Benefits and Uses-Also Send MMS+LiverBal+Quinine - 2.25.21Kirekesztett Magyar HazafiakNessuna valutazione finora
- LUTRONIC 2020 CataolgDocumento13 pagineLUTRONIC 2020 Cataolgkhairul ihsanNessuna valutazione finora
- Hifu 3d-1Documento6 pagineHifu 3d-1sadraNessuna valutazione finora
- Manual Aparato Unoisetion YH-5302Documento17 pagineManual Aparato Unoisetion YH-5302Lily Reyes100% (1)
- Documentos Sobre Probióticos 5Documento9 pagineDocumentos Sobre Probióticos 5Miriam MiguelNessuna valutazione finora
- Documentos Sobre Probióticos 1Documento9 pagineDocumentos Sobre Probióticos 1Miriam MiguelNessuna valutazione finora
- Documentos Sobre Probióticos 3Documento9 pagineDocumentos Sobre Probióticos 3Miriam MiguelNessuna valutazione finora
- Documentos Sobre Probióticos 2Documento5 pagineDocumentos Sobre Probióticos 2Miriam MiguelNessuna valutazione finora
- 1 s2.0 S2405654517302512 MainDocumento9 pagine1 s2.0 S2405654517302512 MainMiriam Miguel100% (1)
- 1 s2.0 S0360301609000467 MainDocumento7 pagine1 s2.0 S0360301609000467 MainMiriam MiguelNessuna valutazione finora
- 1 s2.0 S2405654517302512 MainDocumento9 pagine1 s2.0 S2405654517302512 MainMiriam Miguel100% (1)
- Este Finalmente PDFDocumento8 pagineEste Finalmente PDFMiriam MiguelNessuna valutazione finora
- Daylighting Museums - A Case Study in Lisbon: Fernanda Sá de Oliveira and Manuel Correia GuedesDocumento6 pagineDaylighting Museums - A Case Study in Lisbon: Fernanda Sá de Oliveira and Manuel Correia GuedesMiriam MiguelNessuna valutazione finora
- BaxiDocumento29 pagineBaxiMiriam MiguelNessuna valutazione finora
- Daylighting Museums - A Case Study in Lisbon: Fernanda Sá de Oliveira and Manuel Correia GuedesDocumento6 pagineDaylighting Museums - A Case Study in Lisbon: Fernanda Sá de Oliveira and Manuel Correia GuedesMiriam MiguelNessuna valutazione finora
- 987934Documento5 pagine987934Miriam MiguelNessuna valutazione finora
- Manual Do UsuárioDocumento5 pagineManual Do UsuárioMiriam MiguelNessuna valutazione finora
- Herbal ShampooDocumento8 pagineHerbal ShampooSatpal kumarNessuna valutazione finora
- Life With LucyDocumento4 pagineLife With LucyRobertKienerNessuna valutazione finora
- Changing A Bowel Diversion Ostomy WITH ANSWERDocumento9 pagineChanging A Bowel Diversion Ostomy WITH ANSWERJohn Pearl FernandezNessuna valutazione finora
- Ncp-Impaired S.i.-NavidasDocumento4 pagineNcp-Impaired S.i.-NavidasFran LanNessuna valutazione finora
- Original Article: Clinical and Histopathological Correlation of Cutaneous TuberculosisDocumento6 pagineOriginal Article: Clinical and Histopathological Correlation of Cutaneous Tuberculosisderil ridwanNessuna valutazione finora
- PPT-Snow Algae PowderDocumento45 paginePPT-Snow Algae PowderNG Sze WingNessuna valutazione finora
- NR 20 - Application of Artificial FingernailsDocumento4 pagineNR 20 - Application of Artificial FingernailsCPSSTNessuna valutazione finora
- ModicareDocumento50 pagineModicareNirmalya PurkaitNessuna valutazione finora
- Physical Examination & Review of SystemsDocumento4 paginePhysical Examination & Review of SystemsDexie James Ventenilla DizonNessuna valutazione finora
- 3rd Quarter 5 WeekDocumento30 pagine3rd Quarter 5 WeekFerlizadieflor Fabro De LunasNessuna valutazione finora
- Cosmeticsandtoiletries201905 DLDocumento81 pagineCosmeticsandtoiletries201905 DLrafaeldelperu1982Nessuna valutazione finora
- Hyaluronic Acid by ContiproDocumento2 pagineHyaluronic Acid by Contipro61p2bjx5Nessuna valutazione finora
- Health Condition1Documento22 pagineHealth Condition1Barrack koderaNessuna valutazione finora
- MSDS-Owens Corning-M524-C64 Surface Tissue Page 2Documento1 paginaMSDS-Owens Corning-M524-C64 Surface Tissue Page 2KiranNessuna valutazione finora
- Quantitative Correlation Between Hyaluronic Acid Filler and Hyaluronidase.Documento4 pagineQuantitative Correlation Between Hyaluronic Acid Filler and Hyaluronidase.Lorena AcevedoNessuna valutazione finora
- The Use of Bleach: Guidelines Forcleaning and DisinfectingDocumento3 pagineThe Use of Bleach: Guidelines Forcleaning and DisinfectingAtish KissoonNessuna valutazione finora
- Cenovnik - HemelDocumento4 pagineCenovnik - HemelclassicreviewNessuna valutazione finora
- BURNS BurnDocumento5 pagineBURNS BurnWiljohn de la CruzNessuna valutazione finora
- Lc7 Artificial Teeth 2Documento42 pagineLc7 Artificial Teeth 2Ahmad AbuoddosNessuna valutazione finora
- Case Study IGDocumento2 pagineCase Study IGCheha PaikNessuna valutazione finora
- Titan ShifterDocumento6 pagineTitan ShifterTIAAN VAN DER MERWENessuna valutazione finora
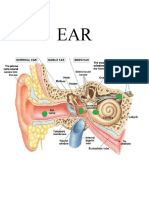
- Anatomy EarDocumento20 pagineAnatomy EarRod HilalNessuna valutazione finora
- DAFTAR HARGA PT. Kimia FarmaDocumento29 pagineDAFTAR HARGA PT. Kimia FarmaAuliaNessuna valutazione finora
- Infant Tub BathDocumento3 pagineInfant Tub Bathako at ang exoNessuna valutazione finora
- 10 Effective Homeopathic Medicines For Pityriasis Alba - DrHomeoDocumento4 pagine10 Effective Homeopathic Medicines For Pityriasis Alba - DrHomeoGer DersenNessuna valutazione finora
- Anwar Spa PamphletDocumento13 pagineAnwar Spa PamphletElNessuna valutazione finora