Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Drug Interactions in Dentistry: Iyad Abou Rabii DDS, Omfs, Mres, PHDDocumento45 pagineDrug Interactions in Dentistry: Iyad Abou Rabii DDS, Omfs, Mres, PHDIyad Abou-Rabii100% (1)
- HealthCare ProvidersDocumento22 pagineHealthCare ProvidersJohn RamosNessuna valutazione finora
- Ade 7 QRT 4Documento4 pagineAde 7 QRT 4Sung Hyo Mi100% (5)
- Ade 7 QRT 4Documento4 pagineAde 7 QRT 4Sung Hyo Mi100% (5)
- 2023 Clinical Guidelines CARES Concept Part IIDocumento20 pagine2023 Clinical Guidelines CARES Concept Part IIMairaMaraviChavezNessuna valutazione finora
- Acls 2017Documento43 pagineAcls 2017DADASDSANessuna valutazione finora
- Mcqs Leadership Management in Nursing 1Documento62 pagineMcqs Leadership Management in Nursing 1henri kaneNessuna valutazione finora
- Colorful 3D Illustrated Remote Learning Events and Special Interest PresentationDocumento9 pagineColorful 3D Illustrated Remote Learning Events and Special Interest PresentationSung Hyo MiNessuna valutazione finora
- Pe Worksheet Dual SportsDocumento7 paginePe Worksheet Dual SportsSung Hyo MiNessuna valutazione finora
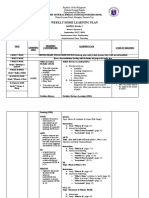
- Weekly Home Learning Plan: MAPEH Grade 7Documento3 pagineWeekly Home Learning Plan: MAPEH Grade 7Sung Hyo MiNessuna valutazione finora
- Camp General Emilio Aguinaldo High School: Individual Workweek Accomplishment ReportDocumento6 pagineCamp General Emilio Aguinaldo High School: Individual Workweek Accomplishment ReportSung Hyo MiNessuna valutazione finora
- Student Remediation PlanDocumento2 pagineStudent Remediation PlanSung Hyo MiNessuna valutazione finora
- Clinic Referral Slip: Camp Gen. Emilio Aguinaldo High School Bonni Serrano Road, Murphy, Quezon CityDocumento1 paginaClinic Referral Slip: Camp Gen. Emilio Aguinaldo High School Bonni Serrano Road, Murphy, Quezon CitySung Hyo MiNessuna valutazione finora
- Lesson Plan PEDocumento2 pagineLesson Plan PESung Hyo MiNessuna valutazione finora
- Selection OF Anterior TeethDocumento20 pagineSelection OF Anterior TeethShivangi PatelNessuna valutazione finora
- Khan Tibbetian Hospital in Nizzamuddin - Google SearchDocumento1 paginaKhan Tibbetian Hospital in Nizzamuddin - Google SearchaaravNessuna valutazione finora
- Form Poa q4 2023 Teddy RevisiDocumento384 pagineForm Poa q4 2023 Teddy RevisiFirdan FauzanYtNessuna valutazione finora
- 1 PBDocumento10 pagine1 PBTsaniya AhdaNessuna valutazione finora
- Association Between Maxillary Posterior Segment Discrepancy and The Angulation of Maxillary Molars in Patients With Different Vertical Growth PatternsDocumento6 pagineAssociation Between Maxillary Posterior Segment Discrepancy and The Angulation of Maxillary Molars in Patients With Different Vertical Growth PatternsFlor GutiérrezNessuna valutazione finora
- Brochure FlowLine Bipore HEPARIN (EN)Documento4 pagineBrochure FlowLine Bipore HEPARIN (EN)Tuyen nguyen ngocNessuna valutazione finora
- BGDES Learners Vaccination Update SY 2022-2023Documento1 paginaBGDES Learners Vaccination Update SY 2022-2023ralpdulayliboonNessuna valutazione finora
- Naturoville Design BriefDocumento6 pagineNaturoville Design BriefAstha SinghNessuna valutazione finora
- 4 Antibacterial Activity of Ethanolic Extract of Hibiscus Rosa Sinensis Flower Against Staphylococcus Epidermidis and Staphylococcus SaprophyticusDocumento12 pagine4 Antibacterial Activity of Ethanolic Extract of Hibiscus Rosa Sinensis Flower Against Staphylococcus Epidermidis and Staphylococcus Saprophyticusrayven casugayNessuna valutazione finora
- Stein. The Influence of Theory On The Psychoanalyst's CountertransferenceDocumento12 pagineStein. The Influence of Theory On The Psychoanalyst's CountertransferenceLeslie MendozaNessuna valutazione finora
- Censo Discapacitados CPT II Ruta 20iiDocumento8 pagineCenso Discapacitados CPT II Ruta 20iikarlais salasNessuna valutazione finora
- Household Covid-19 Vaccination Profiling: City Government of Sorsogon City Health OfficeDocumento2 pagineHousehold Covid-19 Vaccination Profiling: City Government of Sorsogon City Health OfficePee ZeeNessuna valutazione finora
- Occlusal Plane Template TechniqueDocumento39 pagineOcclusal Plane Template TechniqueREWA KAWADENessuna valutazione finora
- Brochure ISDocumento4 pagineBrochure ISJAYESH VIKRAM RastogiNessuna valutazione finora
- General Flight Information: GSO - Strategy, Support and LogisticsDocumento26 pagineGeneral Flight Information: GSO - Strategy, Support and LogisticsIliyanPetrovNessuna valutazione finora
- Intersos Grants ManagerDocumento5 pagineIntersos Grants Managerreem esamNessuna valutazione finora
- Peh 12 w1Documento20 paginePeh 12 w1api-613352174Nessuna valutazione finora
- 476-Article Text-1989-1-10-20210227Documento7 pagine476-Article Text-1989-1-10-20210227ApreliaNessuna valutazione finora
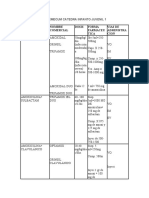
- Antibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionDocumento10 pagineAntibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionLUCRECIA SUAREZ MORENONessuna valutazione finora
- 2022 Employee Benefits Trends: A HR Guide To What's Next For BenefitsDocumento39 pagine2022 Employee Benefits Trends: A HR Guide To What's Next For BenefitsTeoNessuna valutazione finora
- General First Aid QuizDocumento3 pagineGeneral First Aid QuizLucy KiturNessuna valutazione finora
- 1 Burnout in Healthcare: Failure Mode Effects Analysis (FMEA) Associated With Implementation of CDS Tool Into CPOEDocumento5 pagine1 Burnout in Healthcare: Failure Mode Effects Analysis (FMEA) Associated With Implementation of CDS Tool Into CPOEapi-551332616Nessuna valutazione finora
- DocumentDocumento73 pagineDocumentAbdalhakeem AlturkyNessuna valutazione finora
- Kitchen Helper Done 1 PDFDocumento5 pagineKitchen Helper Done 1 PDFDUX Durgesh YadavNessuna valutazione finora
- Silo - Tips Modern PhytotherapistDocumento27 pagineSilo - Tips Modern Phytotherapistagus sangkaNessuna valutazione finora