Potrebbero piacerti anche
- Adult Infectious Disease Bulletpoints HandbookDa EverandAdult Infectious Disease Bulletpoints HandbookValutazione: 4.5 su 5 stelle4.5/5 (9)
- Chlamydia SeminarDocumento110 pagineChlamydia Seminarsuvarnaramesh2007100% (1)
- Cisitcercosis: enfermedad parasitariaDa EverandCisitcercosis: enfermedad parasitariaNessuna valutazione finora
- Super Parasitology TableDocumento11 pagineSuper Parasitology Tablesleepyhead archerNessuna valutazione finora
- Wet MountDocumento25 pagineWet MountJuan Marcos Martinez ZevallosNessuna valutazione finora
- Lecture Rickettsia Chlamydia, MycoplasmaDocumento49 pagineLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- RickettsiaDocumento18 pagineRickettsiaRichard Barrenechea100% (1)
- ISLAB P2 - Anti-Streptolysin ODocumento4 pagineISLAB P2 - Anti-Streptolysin ODanielle Anne LambanNessuna valutazione finora
- Salmonella BasicsDocumento71 pagineSalmonella Basicstummalapalli venkateswara raoNessuna valutazione finora
- Activity 3 - Dna IsolationDocumento4 pagineActivity 3 - Dna IsolationMemeowwNessuna valutazione finora
- Amoebiasis and AmoebaDocumento10 pagineAmoebiasis and AmoebaStephanie Joy EscalaNessuna valutazione finora
- Medical Virology: Introduction To BasicsDocumento88 pagineMedical Virology: Introduction To BasicsSutapa PawarNessuna valutazione finora
- Bates Chapter 8 Lung and ThoraxDocumento15 pagineBates Chapter 8 Lung and ThoraxAdrian CaballesNessuna valutazione finora
- PrionsDocumento28 paginePrionsPaula PollNessuna valutazione finora
- RickettsiaDocumento11 pagineRickettsiaOndape ValeryNessuna valutazione finora
- Virus: Measuring The Size of VirusesDocumento18 pagineVirus: Measuring The Size of VirusesVargheseNessuna valutazione finora
- ENTEROBACTERIACEAEDocumento13 pagineENTEROBACTERIACEAEStephen Jao Ayala Ujano100% (1)
- Immunity To MicrobesDocumento65 pagineImmunity To Microbesmulatumelese100% (1)
- Part Ii Specimen Collection & Laboratory Diagnosis For VirusesDocumento6 paginePart Ii Specimen Collection & Laboratory Diagnosis For VirusesBONNA FAYE CHRISZEL HUI YING TANNessuna valutazione finora
- Rubella - Pediatrics - MSD Manual Professional EditionDocumento4 pagineRubella - Pediatrics - MSD Manual Professional EditionSadia Shafique100% (1)
- 02 Lecture Presentation (Bio20-1, Mapua Institute of Technology)Documento47 pagine02 Lecture Presentation (Bio20-1, Mapua Institute of Technology)Christelle ZuluetaNessuna valutazione finora
- Introduction To VirologyDocumento55 pagineIntroduction To VirologymulatumeleseNessuna valutazione finora
- Introduction To Immunology PDFDocumento15 pagineIntroduction To Immunology PDFanon_143800659100% (1)
- Family of StreptococcaceaeDocumento10 pagineFamily of StreptococcaceaeLovely B. AlipatNessuna valutazione finora
- Micro ExamDocumento7 pagineMicro ExamMarie Llanes100% (1)
- Mycology IntroductionDocumento35 pagineMycology IntroductionDAniq'daNiiq BismaOeyNessuna valutazione finora
- AntigensDocumento24 pagineAntigensUhjafwnuijhnfa KmerkgoeNessuna valutazione finora
- Venipuncture Complications and Preexamination Variables: RequistionsDocumento19 pagineVenipuncture Complications and Preexamination Variables: RequistionsAngel Cascayan Delos SantosNessuna valutazione finora
- Enterobacter With Mucoid Colonies) : Clinical BacteriologyDocumento29 pagineEnterobacter With Mucoid Colonies) : Clinical BacteriologyIra ElizagaNessuna valutazione finora
- Different Types of HazardsDocumento4 pagineDifferent Types of HazardsGNiqM100% (1)
- Morpholofy of MoDocumento44 pagineMorpholofy of MoPathumavathy RamanathanNessuna valutazione finora
- Tests For Dengue GROUP 3Documento22 pagineTests For Dengue GROUP 3chocoholic potchiNessuna valutazione finora
- Immunological Lab Diagnosis of TuberculosisDocumento38 pagineImmunological Lab Diagnosis of TuberculosisRasha EmadNessuna valutazione finora
- Microbiology - Bacteria Summary (Updated)Documento26 pagineMicrobiology - Bacteria Summary (Updated)moZZeltovNessuna valutazione finora
- Mcqs in MicrobiologyDocumento19 pagineMcqs in MicrobiologyTawfeeq AuqbiNessuna valutazione finora
- Hypersensitivity: Dr. Sudheer KherDocumento37 pagineHypersensitivity: Dr. Sudheer KherAbdiladif Ahmed Mohamed100% (1)
- Molbio HandoutDocumento29 pagineMolbio HandoutHazel FlorentinoNessuna valutazione finora
- IMH Laboratory ManualDocumento56 pagineIMH Laboratory ManualHaniya KhanNessuna valutazione finora
- History of Microbiology 16th CENTURYDocumento3 pagineHistory of Microbiology 16th CENTURYMeangel QuillaoNessuna valutazione finora
- Activity 9 Phylum NematodaDocumento18 pagineActivity 9 Phylum Nematodanicole syNessuna valutazione finora
- Infection and Modes of TransmissionDocumento14 pagineInfection and Modes of TransmissionLucky Radita Alma100% (1)
- Bacterial and Viral GeneticsDocumento52 pagineBacterial and Viral GeneticsPradeep Tomar100% (1)
- Diagnostic Microbiology: CampylobacterDocumento25 pagineDiagnostic Microbiology: Campylobacteranon_914901469Nessuna valutazione finora
- Acid Fast Bacteria: M. Tuberculosis, M. LepraeDocumento22 pagineAcid Fast Bacteria: M. Tuberculosis, M. LepraeelaNessuna valutazione finora
- Toxoplasma GondiiDocumento7 pagineToxoplasma GondiiDedy SavradinataNessuna valutazione finora
- Clostrdia: G Positive Spore Forming Anaerobic Toxin Producing RodsDocumento36 pagineClostrdia: G Positive Spore Forming Anaerobic Toxin Producing Rodsjamal nasirNessuna valutazione finora
- Practical Laboratory Diagnosis of Parasitic DiseasesDocumento48 paginePractical Laboratory Diagnosis of Parasitic DiseasesliliposhianNessuna valutazione finora
- 04 Microbiology - Growth, Survival, and Death of MicroorganismsDocumento3 pagine04 Microbiology - Growth, Survival, and Death of MicroorganismsJanet SantosNessuna valutazione finora
- CESTODES Lecture For DM Batch 7Documento73 pagineCESTODES Lecture For DM Batch 7Eliza May BarrettoNessuna valutazione finora
- Introduction To Medical Microbiology, Parasitology & Immunology - Oct 2022Documento16 pagineIntroduction To Medical Microbiology, Parasitology & Immunology - Oct 2022Esther WanjukiNessuna valutazione finora
- Leptospires General Characteristics:: Bacteriology: SpirochetesDocumento5 pagineLeptospires General Characteristics:: Bacteriology: SpirochetesJaellah MatawaNessuna valutazione finora
- Diagnostic Microbiology and Laboratory MethodsDocumento70 pagineDiagnostic Microbiology and Laboratory MethodsArulmany SelliahNessuna valutazione finora
- Group 1 BSMT 3A Act. 5.2Documento7 pagineGroup 1 BSMT 3A Act. 5.2Gennelyn Ross Delos ReyesNessuna valutazione finora
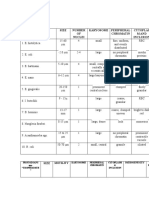
- Table 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionDocumento3 pagineTable 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionJoshua TrinidadNessuna valutazione finora
- Virus Purification: Ricky Fernando Wasista Hanung PujanggaDocumento33 pagineVirus Purification: Ricky Fernando Wasista Hanung PujanggaHanung PujanggaNessuna valutazione finora
- (Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Documento7 pagine(Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Arlene DaroNessuna valutazione finora
- DNA Structure and PropertiesDocumento55 pagineDNA Structure and PropertiesSHARON MARIA SUNNYNessuna valutazione finora
- Neisseria: Family Neisseriaceae With Four GeneraDocumento26 pagineNeisseria: Family Neisseriaceae With Four GeneraAmit Mansukh MistryNessuna valutazione finora
- ChlamydiaDocumento47 pagineChlamydiaAmmarNessuna valutazione finora
- Agent: Defining Characteristics Clinical Diseases Laboratory Diagnosis Treatment SpirochetesDocumento6 pagineAgent: Defining Characteristics Clinical Diseases Laboratory Diagnosis Treatment SpirochetesEd Daniel DavisNessuna valutazione finora
- Meriam Mfc4150 ManDocumento40 pagineMeriam Mfc4150 Manwajahatrafiq6607Nessuna valutazione finora
- Vedic Maths Edited 2Documento9 pagineVedic Maths Edited 2sriram ANessuna valutazione finora
- Nutrition Great Foods For Getting Vitamins A To K in Your DietDocumento1 paginaNutrition Great Foods For Getting Vitamins A To K in Your DietDhruv DuaNessuna valutazione finora
- Lista de Precios Agosto 2022Documento9 pagineLista de Precios Agosto 2022RuvigleidysDeLosSantosNessuna valutazione finora
- Ubi Caritas Guitar Solo Arrangement by Patrick Glenn BalanzaDocumento8 pagineUbi Caritas Guitar Solo Arrangement by Patrick Glenn BalanzaPatrick Glenn BalanzaNessuna valutazione finora
- PH of Soils: Standard Test Method ForDocumento3 paginePH of Soils: Standard Test Method ForYizel CastañedaNessuna valutazione finora
- Automated Dish Washer v1.1Documento21 pagineAutomated Dish Washer v1.1Anonymous XXCCYAEY6M67% (3)
- Research On Export Trade in BangladeshDocumento7 pagineResearch On Export Trade in BangladeshFarjana AnwarNessuna valutazione finora
- Estate TaxDocumento10 pagineEstate TaxCharrie Grace PabloNessuna valutazione finora
- Adime 2Documento10 pagineAdime 2api-307103979Nessuna valutazione finora
- Rubric For Aet570 BenchmarkDocumento4 pagineRubric For Aet570 Benchmarkapi-255765082Nessuna valutazione finora
- Microeconomics Term 1 SlidesDocumento494 pagineMicroeconomics Term 1 SlidesSidra BhattiNessuna valutazione finora
- Benko Gambit-Jacobs and Kinsman, 1999Documento163 pagineBenko Gambit-Jacobs and Kinsman, 1999johnson Greker100% (3)
- Packet Unit 3 - Atomic Structure-Answers ChemistryDocumento11 paginePacket Unit 3 - Atomic Structure-Answers ChemistryMario J. KafatiNessuna valutazione finora
- IPM GuidelinesDocumento6 pagineIPM GuidelinesHittesh SolankiNessuna valutazione finora
- Business CombinationsDocumento18 pagineBusiness Combinationszubair afzalNessuna valutazione finora
- Chapter Three: Tools For Exploring The World: Physical, Perceptual, and Motor DevelopmentDocumento43 pagineChapter Three: Tools For Exploring The World: Physical, Perceptual, and Motor DevelopmentHsieh Yun JuNessuna valutazione finora
- Sistine Chapel Ceiling Lesson PlanDocumento28 pagineSistine Chapel Ceiling Lesson PlannivamNessuna valutazione finora
- Historical Exchange Rates - OANDA AUD-MYRDocumento1 paginaHistorical Exchange Rates - OANDA AUD-MYRML MLNessuna valutazione finora
- A Review of Stories Untold in Modular Distance Learning: A PhenomenologyDocumento8 pagineA Review of Stories Untold in Modular Distance Learning: A PhenomenologyPsychology and Education: A Multidisciplinary JournalNessuna valutazione finora
- Broiler ProductionDocumento13 pagineBroiler ProductionAlexa Khrystal Eve Gorgod100% (1)
- Asan Visa Ae102901499Documento2 pagineAsan Visa Ae102901499hardeep ranaNessuna valutazione finora
- 3rd Page 5Documento1 pagina3rd Page 5api-282737728Nessuna valutazione finora
- OVDT Vs CRT - GeneralDocumento24 pagineOVDT Vs CRT - Generaljaiqc100% (1)
- Progress Report 1Documento3 pagineProgress Report 1api-302815786Nessuna valutazione finora
- Building A Pentesting Lab For Wireless Networks - Sample ChapterDocumento29 pagineBuilding A Pentesting Lab For Wireless Networks - Sample ChapterPackt PublishingNessuna valutazione finora
- Feds Subpoena W-B Area Info: He Imes EaderDocumento42 pagineFeds Subpoena W-B Area Info: He Imes EaderThe Times LeaderNessuna valutazione finora
- Eng21 (Story of Hamguchi Gohei)Documento9 pagineEng21 (Story of Hamguchi Gohei)Alapan NandaNessuna valutazione finora
- ArcGIS Shapefile Files Types & ExtensionsDocumento4 pagineArcGIS Shapefile Files Types & ExtensionsdanangNessuna valutazione finora
- Presentation Municipal Appraisal CommitteeDocumento3 paginePresentation Municipal Appraisal CommitteeEdwin JavateNessuna valutazione finora