Potrebbero piacerti anche
- Ybañez, John Lawrence Q. BSB2-B Asin LawDocumento5 pagineYbañez, John Lawrence Q. BSB2-B Asin LawJohn Lawrence YbanezNessuna valutazione finora
- Operative Obstetrics: Nursing InterventionsDocumento7 pagineOperative Obstetrics: Nursing InterventionsJohn Lawrence YbanezNessuna valutazione finora
- Care of Mother, Child, and Adolescent (Well-Client) Related Learning Experience, Skills LaboratoryDocumento7 pagineCare of Mother, Child, and Adolescent (Well-Client) Related Learning Experience, Skills LaboratoryJohn Lawrence YbanezNessuna valutazione finora
- CHN Process NotesDocumento9 pagineCHN Process NotesJohn Lawrence YbanezNessuna valutazione finora
- Water and Electrolytes NOTESDocumento108 pagineWater and Electrolytes NOTESJohn Lawrence YbanezNessuna valutazione finora
- Production of Reproductive Hormones: NCM 107 NotesDocumento5 pagineProduction of Reproductive Hormones: NCM 107 NotesJohn Lawrence YbanezNessuna valutazione finora
- Ybañez, John Lawrence Q BSN2-BDocumento2 pagineYbañez, John Lawrence Q BSN2-BJohn Lawrence YbanezNessuna valutazione finora
- Nursing Process Worksheet 2020Documento1 paginaNursing Process Worksheet 2020John Lawrence Ybanez100% (1)
- Common Special Types of BedDocumento14 pagineCommon Special Types of BedJohn Lawrence Ybanez100% (1)
- Nursing Theorist: Lydia Hall: Dexter R. Gromia BSN 1-J TFNDocumento4 pagineNursing Theorist: Lydia Hall: Dexter R. Gromia BSN 1-J TFNJohn Lawrence YbanezNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- His Tory of ODDocumento13 pagineHis Tory of ODAmar NathNessuna valutazione finora
- Nme 427 1meDocumento33 pagineNme 427 1meAriel Gamboa100% (1)
- Hunna I. Lipke v. City of New York, Et Al.Documento21 pagineHunna I. Lipke v. City of New York, Et Al.Eric SandersNessuna valutazione finora
- User Manual: Women and Child Development DepartmentDocumento27 pagineUser Manual: Women and Child Development Department2271 Nitish GuptaNessuna valutazione finora
- Standards of Care in Diabetes-2023: 14. Children and AdolescentsDocumento24 pagineStandards of Care in Diabetes-2023: 14. Children and AdolescentsFranklin MatuteNessuna valutazione finora
- Resultados SaludDignaDocumento2 pagineResultados SaludDignaAdriana RamosNessuna valutazione finora
- Theories and Principle of Health Care EthicsDocumento6 pagineTheories and Principle of Health Care EthicspeachyskizNessuna valutazione finora
- Detailed Lesson Plan in Health10 Final 1Documento7 pagineDetailed Lesson Plan in Health10 Final 1nezziele asisNessuna valutazione finora
- Supplementary Notes On MT130 Module 1 and 2Documento18 pagineSupplementary Notes On MT130 Module 1 and 2Junaid AkhtarNessuna valutazione finora
- Maternity and Women Health Care 10th Edition Lowdermilk Test BankDocumento13 pagineMaternity and Women Health Care 10th Edition Lowdermilk Test Banklilyadelaides4zo100% (31)
- Jurnal PKM Upaya Pencapaian Herd ImmunityDocumento7 pagineJurnal PKM Upaya Pencapaian Herd ImmunityMardhiyah AfriniNessuna valutazione finora
- Vertise Flow CompositeDocumento24 pagineVertise Flow Compositeionut1ilie-1Nessuna valutazione finora
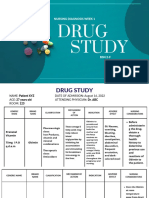
- Study: Nursing Diagnosis Week 1Documento9 pagineStudy: Nursing Diagnosis Week 122 - Fernandez, Lyza Mae D.Nessuna valutazione finora
- Usp 〈1029〉 Good Documentation Guidelines良好文件指南(中英双语)Documento13 pagineUsp 〈1029〉 Good Documentation Guidelines良好文件指南(中英双语)lewis liNessuna valutazione finora
- Toxins of Molds From: Decaying TomatoDocumento8 pagineToxins of Molds From: Decaying TomatoOlatunbosun OyeyemiNessuna valutazione finora
- L1-M02-02 - 03-P - Work Punctuality BehaviourDocumento6 pagineL1-M02-02 - 03-P - Work Punctuality BehaviourDEATH 16YNessuna valutazione finora
- Online Rules and Regulations: QR-ACA-CAE04-002Documento51 pagineOnline Rules and Regulations: QR-ACA-CAE04-002Loren Marie Lemana AceboNessuna valutazione finora
- Amjad Iqbal: ObjectiveDocumento17 pagineAmjad Iqbal: ObjectiveKhalid HussainNessuna valutazione finora
- Review of Literature Related To Kangaroo Mother CareDocumento8 pagineReview of Literature Related To Kangaroo Mother Carec5swkkcnNessuna valutazione finora
- Community Health Survey ToolDocumento3 pagineCommunity Health Survey ToolMarjune DimayugaNessuna valutazione finora
- CNS Stimulants: College of Pharmacy Department of PharmacologyDocumento20 pagineCNS Stimulants: College of Pharmacy Department of PharmacologyDrDeepak PrasharNessuna valutazione finora
- Article HealthDocumento3 pagineArticle Healthkaii cutieNessuna valutazione finora
- Final Thesis PDFDocumento81 pagineFinal Thesis PDFAdnanNessuna valutazione finora
- Republic of The Philippines: Scale Projects Are Defined As Those Construction Projects That Are Intended For PurelyDocumento12 pagineRepublic of The Philippines: Scale Projects Are Defined As Those Construction Projects That Are Intended For PurelyBobby Olavides SebastianNessuna valutazione finora
- FOA GROUP 1 Merck CaseDocumento45 pagineFOA GROUP 1 Merck CaseKSNessuna valutazione finora
- Aims Email Ids - DoctorsDocumento10 pagineAims Email Ids - DoctorsKunwar SaigalNessuna valutazione finora
- USP Initiatives in Promoting The Quality of Medicines GloballyDocumento33 pagineUSP Initiatives in Promoting The Quality of Medicines GloballyMiles MudzvitiNessuna valutazione finora
- Abundance Script - PDF-45-49Documento5 pagineAbundance Script - PDF-45-49patrickchatezviNessuna valutazione finora
- SUMMER 2013 Kripalu Catalog: Bikram ChoudhuryDocumento116 pagineSUMMER 2013 Kripalu Catalog: Bikram ChoudhuryBikram ChoudhuryNessuna valutazione finora
- The Development and Validation of A Dissolution Method For Clomipramine Solid Dosage FormsDocumento7 pagineThe Development and Validation of A Dissolution Method For Clomipramine Solid Dosage FormsBad Gal Riri BrunoNessuna valutazione finora