Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Sociology Chapter 1Documento30 pagineSociology Chapter 1Joanne Tolentino100% (1)
- Suicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideDocumento12 pagineSuicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideShreeya GhagNessuna valutazione finora
- Indian Recipes CombinedDocumento174 pagineIndian Recipes CombinedNarendra TomarNessuna valutazione finora
- Unit 4 Practice TestDocumento11 pagineUnit 4 Practice TestMatt JonesNessuna valutazione finora
- PerDev Q1 Module 2 Developing The Whole Person Ver1-ForCADILLADocumento33 paginePerDev Q1 Module 2 Developing The Whole Person Ver1-ForCADILLAJenny E. Forcadilla100% (4)
- Reading & Writing QUIZ 1Documento3 pagineReading & Writing QUIZ 1Marissa UrnosNessuna valutazione finora
- Anthropometrics ErgonomicsDocumento78 pagineAnthropometrics ErgonomicsashokdinoNessuna valutazione finora
- Spark AR Open Program - BrochureDocumento1 paginaSpark AR Open Program - BrochureashokdinoNessuna valutazione finora
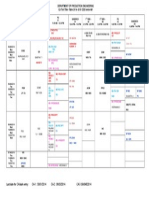
- Time Table Even 2017 2018Documento1 paginaTime Table Even 2017 2018ashokdinoNessuna valutazione finora
- Current Techniques For Assessing Physical Exposure To Work Related Musculoskeletal Risks With Emphasis On Posture Based MethodsDocumento23 pagineCurrent Techniques For Assessing Physical Exposure To Work Related Musculoskeletal Risks With Emphasis On Posture Based MethodsashokdinoNessuna valutazione finora
- CA 01 Test Timetable (Senior) ODD 14-15Documento1 paginaCA 01 Test Timetable (Senior) ODD 14-15ashokdinoNessuna valutazione finora
- MKT201 IndiDocumento8 pagineMKT201 IndiPhạm Thu HằngNessuna valutazione finora
- How Diversity Makes Us Smarter - Greater GoodDocumento9 pagineHow Diversity Makes Us Smarter - Greater GoodSafa ShujaNessuna valutazione finora
- HIstory of PsychologyDocumento3 pagineHIstory of PsychologyMICAELLA TABUENANessuna valutazione finora
- Smart Goals Worksheet 4Documento1 paginaSmart Goals Worksheet 4api-330070899Nessuna valutazione finora
- Introduction To The Study of Consumer BehaviorDocumento22 pagineIntroduction To The Study of Consumer BehaviorTuhina MistryNessuna valutazione finora
- SDLP - Nativist TheoryDocumento6 pagineSDLP - Nativist TheoryDinah DimagibaNessuna valutazione finora
- Lego TherapyDocumento6 pagineLego TherapyToni ErdfeldNessuna valutazione finora
- M4L1 Handout Activity5Documento3 pagineM4L1 Handout Activity5Kaiden Kena RhemNessuna valutazione finora
- A. AC Caring and AdvocacyDocumento47 pagineA. AC Caring and AdvocacyAnuchithra RadhakrishnanNessuna valutazione finora
- Ipgm Muet Writing Question 2-1Documento42 pagineIpgm Muet Writing Question 2-1g-ipgp202723612Nessuna valutazione finora
- PledgeDocumento3 paginePledgeGillian Faye LechocoNessuna valutazione finora
- 2019年12月六级真题(第1套)Documento11 pagine2019年12月六级真题(第1套)六级真题及解析(1990-2022)Nessuna valutazione finora
- Bus 5113 Discussion Unit 6Documento4 pagineBus 5113 Discussion Unit 6Joseph KamaraNessuna valutazione finora
- JASA, San Matias, Guagua, PampangaDocumento4 pagineJASA, San Matias, Guagua, PampangaPoison IvyNessuna valutazione finora
- Resume MohdDocumento2 pagineResume Mohdkeez72Nessuna valutazione finora
- Activity WorkbookDocumento21 pagineActivity Workbookmendozacruzadojosue.Nessuna valutazione finora
- The Emerging Field of Conservation Psychology: Carol D. SaundersDocumento13 pagineThe Emerging Field of Conservation Psychology: Carol D. SaundersMilfor WolfpofNessuna valutazione finora
- FH Food Security Program Lifecycle Toolkit Manual 07 JulyDocumento169 pagineFH Food Security Program Lifecycle Toolkit Manual 07 JulyMohamed AbdiNessuna valutazione finora
- Parent-Child Rating Scale (PCRS) : A Parent-Reported Questionnaire To Assess Social and Emotional Functioning in ChildrenDocumento28 pagineParent-Child Rating Scale (PCRS) : A Parent-Reported Questionnaire To Assess Social and Emotional Functioning in ChildrenEleenaNessuna valutazione finora
- Pushes and Pulls Forces Lesson Plan GGDocumento3 paginePushes and Pulls Forces Lesson Plan GGMohammadNessuna valutazione finora
- Grade RemarksDocumento1 paginaGrade RemarksMishaam VirkNessuna valutazione finora
- G I Ý Speaking Part 2,3 Quí 3 2022 (Full)Documento88 pagineG I Ý Speaking Part 2,3 Quí 3 2022 (Full)꧁Lilie꧂Nessuna valutazione finora
- Resource 4: Applying Ethical Frameworks in Practice Grading RubricDocumento5 pagineResource 4: Applying Ethical Frameworks in Practice Grading RubricJhunalyn Hazze TizonNessuna valutazione finora
- IN6 Hold 2 Out 7: 10-Minute Toughness Summary WorksheetDocumento6 pagineIN6 Hold 2 Out 7: 10-Minute Toughness Summary WorksheetmrpablosanchezNessuna valutazione finora
- Paper 3 Final Exam Global Citizenship Vs National CitizenshipDocumento3 paginePaper 3 Final Exam Global Citizenship Vs National CitizenshipAlliahkherzteen LagoNessuna valutazione finora