Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Polycystic Ovary Syndrome - A Common Reproductive Syndrome With Long-Term Metabolic Consequences
Caricato da
KopeDescrizione originale:
Titolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Polycystic Ovary Syndrome - A Common Reproductive Syndrome With Long-Term Metabolic Consequences
Caricato da
KopeCopyright:
Formati disponibili
CME Review Article
Polycystic ovary syndrome: a common
reproductive syndrome with long-term
metabolic consequences
Tiffany TL Yau, Noel YH Ng, LP Cheung, Ronald CW Ma *
ABSTRACT focus on the specific needs of the individual, and
may change according to different stages of the life
Polycystic ovary syndrome is the most common
course. In view of the clinical manifestations of the
endocrine disorder among women of reproductive
condition, there is recent debate about whether
age. Although traditionally viewed as a reproductive
the current name is misleading, and whether
disorder, there is increasing appreciation that it
the condition should be renamed as metabolic
is associated with significantly increased risk of
reproductive syndrome.
cardiometabolic disorders. Women with polycystic
ovary syndrome may present to clinicians via a
variety of different routes and symptoms. Although
Hong Kong Med J 2017;23:622–34
the impact on reproduction predominates during the
DOI: 10.12809/hkmj176308
reproductive years, the increased cardiometabolic
problems are likely to become more important at 1
TTL Yau #, FHKCP, FHKAM (Medicine)
later stages of the life course. Women with polycystic 1
NYH Ng #, BSc, MRes
ovary syndrome have an approximately 2- to 5-fold 2
LP Cheung, FRCOG, FHKAM (Obstetrics and Gynaecology)
increased risk of dysglycaemia or type 2 diabetes, and 1,3
RCW Ma *, FRCP, FHKAM (Medicine)
hence regular screening with oral glucose tolerance #
TT Yau and NY Ng have equal contribution in this study.
test is warranted. Although the diagnostic criteria
for polycystic ovary syndrome are still evolving and 1
Department of Medicine and Therapeutics, The Chinese University of
are undergoing revision, the diagnosis is increasingly Hong Kong, Shatin, Hong Kong
focused on the presence of hyperandrogenism, with 2
Department of Obstetrics and Gynaecology, The Chinese University of
Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong
the significance of polycystic ovarian morphology 3
Hong Kong Institute of Diabetes and Obesity, The Chinese University of
This article was in the absence of associated hyperandrogenism or Hong Kong, Shatin, Hong Kong
published on 24 Nov anovulation remaining uncertain. The management
2017 at www.hkmj.org. of women with polycystic ovary syndrome should * Corresponding author: rcwma@cuhk.edu.hk
Introduction experienced a diagnostic delay in excess of 2 years.5
Polycystic ovary syndrome (PCOS) was first Diagnosis of polycystic ovary
described by Stein and Leventhal in 1935,1 when
they noted an association between the presence of
syndrome: historical aspects and
bilateral polycystic ovaries and signs of amenorrhoea, evolution of diagnostic criteria
oligomenorrhoea, hirsutism, and obesity. It is now Polycystic ovary syndrome is considered to be
recognised as one of the most common endocrine a heterogeneous disorder with multifactorial
disorders of women, affecting between 6% and 12% cause. The principal features of PCOS include
of women overall.2 A study in southern Chinese hyperandrogenism, oligomenorrhoea, and/or
reported a prevalence of 2.2% among women of polycystic ovaries. There have been several proposed
reproductive age.3 The prevalence can be as high diagnostic criteria for PCOS as described in Table
as 70% to 80% in women with oligoamenorrhoea 1.6-9 All criteria require exclusion of other disorders
and 60% to 70% in women with anovulatory that may mimic the clinical features of PCOS, such
infertility. Women with PCOS have an increased as thyroid dysfunction, hyperprolactinaemia, non-
risk of gynaecological, reproductive, medical and classic congenital adrenal hyperplasia (CAH), and
sleep problems, and hence are at risk of increased Cushing’s syndrome.
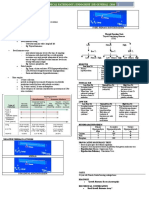
morbidities across the life course (Fig 1).4 Despite The prevalence of PCOS depends on the
being a common condition, however, the presenting diagnostic criteria used to define the disorder. To
features of PCOS are often not recognised, resulting date, the prevalence of PCOS has been determined
in a delay in diagnosis. In a recent international primarily using the National Institutes of Health
survey, approximately half of the women with PCOS 1990 criteria. A summary report from the National
consulted three or more health care providers before Institutes of Health Evidence-based Methodology
the diagnosis was made, and more than one third Workshop on PCOS in December 2012 concluded
622 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
that the Rotterdam criteria should be adopted for
now because it is the most inclusive.10 Using the 多囊卵巢綜合症:常見的生殖內分泌
Rotterdam criteria, many patients can be diagnosed
based on the history and physical examination (eg 代謝異常疾病
a history of irregular menses, and clinical signs of 丘芷苓、吳逸晞、張麗冰、馬青雲
hyperandrogenism). The panel also suggested that 多囊卵巢綜合症是生育年齡婦女中最常見的內分泌紊亂疾病。雖然傳
the disorder should be renamed to more adequately 統上被視為一種生殖障礙,但人們越發意識到此症可能會增加心臟代
reflect the complex metabolic, hypothalamic, 謝異常的風險。多囊卵巢綜合症患者可能會出現不同種類的症狀。雖
pituitary, ovarian, and adrenal interactions that 然此症會在生育期內影響患者懷孕的機會,事實上它在往後的日子增
characterise the syndrome. A previous local study 加患者心臟代謝的問題更不容忽視。多囊卵巢綜合症患者患有血糖異
by Lam et al11 comparing the different diagnostic 常或II型糖尿病的風險增加約2至5倍,因此有必要定期進行口服葡萄
criteria in Hong Kong Chinese women concluded 糖耐量測試的檢測。雖然多囊卵巢綜合症的診斷標準仍在發展階段,
that the Rotterdam criteria are generally applicable 亦不斷進行修訂,但診斷越見集中在雄激素過多的層面。在沒有雄激
to our population. Nevertheless, recent discussion 素過多或持續無排卵的情況下,多形性卵巢形態是否重要仍具爭論。
has centred on the importance of hyperandrogenism, 治理多囊卵巢綜合症的婦女應根據個別患者的需要,也可能會隨着患
and emerging evidence suggests that women with 者的年齡而改變。鑑於病情的臨床表現,最近有關此症存在爭辯,包
radiological evidence of polycystic ovaries, but 括其名稱是否誤導,以及應否改名為代謝性生殖綜合症。
no other clinical features of PCOS, represent a
population generally of lower risk who are distinct
from other women with PCOS who fulfil current
diagnostic criteria.12
Prenatal Childhood Adolescence Reproductive Postmenopausal
Pathogenesis
Menstrual
To date, the pathophysiology of PCOS remains Premature irregularities
adrenarche
unclear; yet, substantial evidence suggests it is
Infertility
a multifactorial condition, where interactions Reproductive Endometrial
between endocrine, metabolic, genetic, and cancer
environmental factors intrinsic to each other act
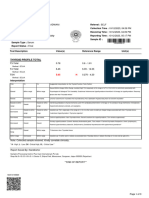
in consonance towards a common result (Fig 2).13,14 Acne
Endocrine
Also, the heterogeneity of PCOS further reinforces Hirsutism
its multifactorial nature. Although familial
Impaired glucose tolerance
segregation of cases suggests a genetic component
in this syndrome, most of the susceptibility genes Gestational diabetes, type 2 diabetes
and single-nucleotide polymorphisms remain to Cardio- Dyslipidaemia
metabolic
be discovered.15,16 Among its diverse phenotypes, Hypertension
hyperandrogenism and ovarian dysfunction are Non-alcoholic fatty liver disease
recognised as the two main features of PCOS.6,16 Cardiovascular
Hyperandrogenism in PCOS is recognised as the disease
excessive androgen biosynthesis, use, and meta- FIG 1. Impacts of polycystic ovary syndrome on reproductive, endocrine, and
bolism. When the ovaries are stimulated to produce cardiometabolic outcome across the life course
excessive amounts of androgen, an accumulation of
numerous follicles or cysts can be observed in the
ovary. Insulin resistance is also a major cause of
hyperandrogenism in PCOS, through stimulating the
(LH) can lead to an increase in androgen production
secretion of ovarian androgen and inhibiting hepatic
by the ovarian thecal cells. This is thought to be due to
sex hormone–binding globulin (SHBG) production.17
increased gonadotropin-releasing hormone (GnRH)
Approximately 80% to 85% of women with clinicalpulse frequency, resulting in increased frequency
hyperandrogenism have PCOS.8,18 Women with and pulsatile secretion of LH, and increased levels
PCOS and hyperandrogenism may experience excessof LH relative to follicle-stimulating hormone (FSH)
hair growth, acne, and/or abnormal folliculogenesis.
in the circulation.14,19,20 There also appears to be
Three major pathophysiological pathways have been
resistance to the negative feedback by progesterone
described, but they are not mutually exclusive. They
to the GnRH pulse generator, which is often present
are ovulatory dysfunction, disordered gonadotropin
by puberty. The increased LH/FSH ratio, along with
release, and insulin resistance. some ovarian resistance to FSH, results in excess
production of androgens from thecal cells in ovarian
Disordered gonadotropin release and excess follicles, leading to impaired follicular development,
androgen release and reduced inhibition of the GnRH pulse generator
In PCOS, hypersecretion of luteinising hormone by progesterone, thereby setting up a vicious cycle
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 623
# Yau et al #
TABLE 1. Summary of proposed diagnostic criteria for PCOS in adults6-9 *
Criteria National Rotterdam Androgen Excess
Institutes of (2003)— and PCOS
Health (1990)6 diagnosis Society (2009)—
established if 2 diagnosis requires
out of 3 criteria hyperandrogenism
are met7 with 1 of 2
remaining criteria8
Hyperandrogenism Clinical hyperandrogenism + +/- +
• Acne or hirsutism or androgenic alopecia
and/or
Biochemical hyperandrogenism
• Elevated serum androgen level (total testosterone or
bioavailable testosterone or free testosterone)†
Oligo-anovulation • ≤8 Menstrual cycles per year, or frequent bleeding at intervals + +/- +/-
<21 days, or infrequent bleeding at intervals >35 days
• Mid-luteal progesterone documenting anovulation
Polycystic ovary • >12 Follicles of 2-9 mm in diameter in at least one ovary Not required +/- +/-
(without a cyst or dominant follicle), and/or
• Ovarian volume >10 mL
Abbreviation: PCOS = polycystic ovary syndrome
* Legend: + indicates an essential criterion for diagnosis; +/- indicates clinical features that are one of the criteria which may need to be present for the
diagnosis to be established
† Given the variability in testosterone level and the suboptimal standardisation of assays, it is difficult to define an absolute level that is diagnostic of PCOS
or other causes of hyperandrogenism, and the Task Force recommends familiarity with cut-offs of local assays9
Insulin resistance
Altered caused by:
Hypothalamus
Hypothalamic neurons adipocytokines • genetic
• environment
Hypothalamus
• obesity
Inflowing
blood
Portal
blood
Increased GnRH Adipose • adipocyte
Anterior
vessels
pulse frequency tissue dysfunction
pituitary
Pituitary Posterior
pituitary
Pancreas
FSH LH Progesterone
Hyperinsulinaemia
Liver
Hyperandrogenism ↓ SHBG
↑ LH/FSH ratio
↑ TG
↑ DHEAS production
↑ IGF-1 ↓ IGFBP-1 ↑ Cholesterol
Adrenal
gland
With ↑ LH
Theca cell Follicular arrest
leading to PCOM
Androgen
Granulosa cell
Ovary
Oestrogen
FIG 2. Pathophysiology of polycystic ovary syndrome
Abbreviations: DHEAS = dehydroepiandrosterone sulfate; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; IGF-1 = insulin-like
growth factor 1; IGFBP-1 = insulin-like growth factor–binding protein-1; LH = luteinising hormone; PCOM = polycystic ovarian morphology; SHBG = sex
hormone–binding globulin; TG = triglycerides
624 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
that exacerbates the hypersecretion of LH, and among lean patients with PCOS, but this is further
ovulatory dysfunction.14,19,20 exacerbated in the presence of obesity.39,40
A stepwise increase in the prevalence of
Ovulatory dysfunction glucose intolerance with increasing body mass index
(BMI) has been described in cross-sectional studies
Unlike the ovarian follicular development in healthy performed in women with this disorder.41 Although
women, in PCOS cases, follicle growth is disrupted most women with PCOS have normal insulin
due to ovarian hyperandrogenism, hyperinsulinaemia secretory responsiveness, studies have suggested
from insulin resistance, and intra-ovarian paracrine that PCOS women, particularly those with a family
signalling. Hyperinsulinaemia further impairs follicle history of type 2 diabetes (T2D), have impaired
growth by amplifying LH-stimulated and insulin- β-cell function or a subnormal disposition index (an
like growth factor 1 (IGF-1)–stimulated androgen index of β-cell function that takes insulin resistance
production.21-24 Hyperinsulinaemia also elevates into account).16,42,43
serum free testosterone levels through decreased
hepatic SHBG production, and enhances serum Adipose dysfunction
IGF-1 bioactivity through suppression of IGF-binding
Although the full molecular mechanisms underlying
protein production.25 Insulin excess also promotes
insulin resistance in PCOS remain unclear, primary
premature follicle luteinisation through enhanced
defects in insulin-medicated glucose transport,44
FSH-induced granulosa cell differentiation, which
GLUT4 production,45 and insulin or adrenergic
arrests granulosa cell proliferation and subsequent
regulated lipolysis46 in adipocytes (and sometimes
follicle growth.26 Finally, overproduction of anti-
in myocytes and fibroblasts) have been reported.
Müllerian hormone (AMH)27-29 by the granulosa cells
Insulin resistance in PCOS contributes to the
of ovarian follicles in PCOS appears to antagonise
dysfunctional adipogenesis to some degree from an
FSH action in small PCOS follicles. The relatively
30
impaired capacity of regional adipose tissue storage
lower FSH levels contribute to arrested follicular
to properly expand with increased dietary caloric
development in the ovary, leading to amenorrhoea,
intake.47-49 Adipose tissue secretes numerous factors
anovulation, and polycystic morphology. 8,16
to regulate metabolic function, appetite, neural
activity, and digestion. This tissue is also heavily
Insulin resistance infiltrated by macrophages, and a crosstalk exists
In PCOS cases, there is an increased level of between adipocytes, macrophages, and pluripotent
bioavailable androgens that leads to increased insulin cells for complex paracrine interactions. It is known
resistance in peripheral tissues (mostly in the skeletal that dysregulation of adipokine production, such
muscle).31 Insulin resistance causes compensatory as adiponectin, by macrophage-secreted cytokines
hyperinsulinaemia and might contribute to in PCOS facilitates the development of insulin
hyperandrogenism and gonadotropin aberrations resistance.50 Other adipokines including leptin,
through several mechanisms. Insulin may act retinol-binding protein 4, and visfatin have also
directly in the hypothalamus, the pituitary or both been implicated.51 Improved understanding of the
and thereby contribute to abnormal gonadotropin underlying mechanisms that govern adipose tissue
levels. By facilitating the stimulatory role of LH, dysfunction and insulin resistance in PCOS would be
hyperinsulinaemia leads to further increase in beneficial in the identification of novel therapeutic
ovarian androgen production in theca calls.32 High targets for PCOS and other related disorders.16
insulin can also serve as a co-factor to stimulate
adrenocorticotropic hormone–mediated androgen Intrauterine environment
production in the adrenal glands.33 Moreover, an In humans, rhesus monkeys and sheep, inappropriate
insulin-induced decrease in the production of SHBG testosterone exposure during fetal life alters the
in the liver increases the amount of free bioavailable developmental trajectory of the female leading
androgens.34 to PCOS-like phenotypes, such as phenotypic
Most women with PCOS, particularly those masculinisation; reproductive, neuroendocrine,
who are overweight or obese, do in fact have insulin ovarian disruptions; and hyperinsulinaemia.52 In
resistance and compensatory hyperinsulinaemia,35,36 a human study, it has been shown that there is an
partly attributable to an intrinsic insulin resistance increased prevalence of PCOS in women with classic
mechanism.36-38 CAH and congenital adrenal virilising tumours.53
Using the homeostasis model assessment, 50% In one human study, higher testosterone levels
to 70% of women with PCOS demonstrate insulin compared with those usually observed in normal
resistance. Using the gold standard technique females were found in the umbilical vein of female
of euglycaemic hyperinsulinaemic clamp, it was infants born to mothers with PCOS54; yet, another
found that PCOS exhibits insulin resistance that prospective study that investigated the relationship
is independent of obesity, and is present even between prenatal androgen exposure and the
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 625
# Yau et al #
development of PCOS in female adolescence did not Clinical features and
confirm any association between these variables.55
Excess fetal exposure to maternal androgens
co-morbidities
is thought to contribute to induction of the PCOS Gynaecological and reproductive
phenotype in offspring/children. Nonetheless, more dysfunction
clinical studies are needed to confirm the role of Menstrual dysfunction is common and is
intrauterine androgen exposure on human fetal characterised by oligomenorrhoea and, less often,
development. amenorrhoea. Nonetheless, menstrual problems are
frequently neglected and anovulatory infertility is
Recent insights from genetic studies frequently the initial complaint for which the patient
Polycystic ovary syndrome has a high heritability seeks medical advice. Women with PCOS have an
of approximately 80%. Although a large number of increased risk of miscarriage, gestational diabetes,
candidate gene studies have been conducted, no pre-eclampsia, and preterm labour.58-60 A meta-
genetic variants have been found to be consistently analysis highlighted that the risks of gestational
associated with PCOS. Recent hypothesis-free diabetes, pregnancy-induced hypertension, and pre-
genome-wide association studies using high-density eclampsia are approximately 3-fold, whereas the risk
genotyping arrays that systematically investigate for preterm labour is approximately 2-fold among
common variants across the genome have identified women with PCOS.58 The reasons for the adverse
several genetic loci to be significantly associated pregnancy outcomes are unclear, but hypersecretion
with PCOS (Table 2).56 These have shed light on of LH, hyperandrogenaemia and hyperinsulinaemia
the important role of the gonadotropin axis in the have all been postulated. Due to anovulatory
pathogenesis of PCOS, as well as several other dysfunction and consequent long-term unopposed
novel pathways, including epidermal growth factor oestrogen stimulation, PCOS patients are at
signalling. Interestingly, genetic studies have increased risk of endometrial cancer.61,62 Nonetheless,
revealed a significant overlap of findings when there is currently no consensus to support routine
different diagnostic criteria of PCOS have been biopsy or ultrasound of the endometrium for endo-
applied, highlighting greater homogeneity than metrial hyperplasia or cancer screening in asymp-
previously appreciated.16,56,57 tomatic women due its poor diagnostic accuracy.63
TABLE 2. Genetic loci associated with polycystic ovary syndrome discovered in genome-wide association studies56
Chromosome Nearest gene GWAS top SNP Odds ratio P value Discovery population Replicated population(s)
2p16.3 LHCGR rs13405728 1.41 7.55 x 10-21 Chinese Europeans, Indians
2p16.3 FSHR rs2268361 1.15 9.89 x 10 -13
Chinese Europeans, Arabs, Chinese
2p21 THADA rs13429458 1.49 1.73 x 10 -23
Chinese Europeans, Chinese
2q34 ERBB4 rs1351592 1.18 1.2 x 10-12 Chinese -
5q31.1 RAD50 rs13164856 1.13 3.5 x 10 -9
Chinese -
8p32.1 GATA4 rs804279 1.35 8.0 x 10-10 Chinese -
9q33.3 DENND1A rs2479106 1.34 8.12 x 10 -19
Chinese Europeans
9q22.32 C9orf3 rs4385527 1.19 5.87 x 10 -9
Chinese Chinese, Europeans
rs3802457 1.30 5.28 x 10-14 Chinese -
11p14.1 FSHB rs11031006 1.16 1.9 x 10 -8
European Europeans, Chinese
11q22.1 YAP1 rs1894116 1.27 1.08 x 10-22 Chinese Europeans, Chinese
rs11225154 1.22 7.6 x 10-11 European Chinese
12q14.3 HMGA2 rs2272046 1.43 1.95 x 10-21 Chinese Europeans
12q13.2 RAB5B/SUOX rs705702 1.27 8.64 x 10-26 Chinese Europeans
12q21.2 KRR1 rs1275468 1.13 1.9 x 10 -8
Europeans -
16q12.1 TOX3 rS4784165 1.15 3.64 x 10-11 Chinese Europeans
19p13.3 INSR rs2059807 1.14 1.09 x 10-8 Chinese Europeans
20q13.2 SUMO1P1 rs6022786 1.13 1.83 x 10-9 Chinese -
Abbreviations: GWAS = genome-wide association study; SNP = single-nucleotide polymorphism
626 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
Endocrine dysfunction 2-fold increase in risk of cardiovascular diseases.72 A
Women with PCOS have varying degrees and cross-sectional study evaluated the cardiometabolic
manifestations of androgen excess. Clinical signs of risk factors in 295 Hong Kong Chinese women with
hyperandrogenism include acne, hirsutism, male- PCOS with a mean age of 30 years.68 It found that
pattern hair loss, and/or elevated serum androgen the prevalence of metabolic syndrome in this cohort
concentrations. Hirsutism is the most common was 24.9% despite their relatively young age, a 5-fold
symptom of hyperandrogenism, affecting up to 70% increase in risk compared with women without
of women with PCOS. It is commonly noted on the PCOS even after controlling for age and BMI.68 In
upper lip, chin, periareolar area, in the mid-sternum, another study involving 170 Asian women with
and along the linea alba of the lower abdomen. There PCOS, metabolic syndrome as defined according to
is substantial ethnic variation in hirsutism where the International Diabetes Federation criteria was
Asian women with PCOS have a lesser degree of present in 35.3% of the subjects.73
hirsutism.8 Signs of more severe androgen excess— The prevalence of non-alcoholic fatty liver
such as deepening of the voice, breast atrophy, disease (including non-alcoholic steatohepatitis),
and clitoromegaly—occur rarely and suggest the and obstructive sleep apnoea is also increased in
possibility of ovarian hyperthecosis or an androgen- women with PCOS. Even after controlling for BMI,
secreting tumour. women with PCOS are still 30 times more likely to
have sleep-disordered breathing and 9 times more
likely than controls to have daytime sleepiness.74,75
Metabolic dysfunction and cardiovascular The presence of obesity, insulin resistance,
risks impaired glucose tolerance (or T2D), and
Polycystic ovary syndrome is associated with dyslipidaemia may predispose women with PCOS to
cardiovascular risk factors, including obesity, coronary heart disease. An excess risk of coronary
hypertension, glucose intolerance, dyslipidaemia, heart disease or stroke in women with PCOS,
and obstructive sleep apnoea.64 The high prevalence however, is not well established due to the lack of
of metabolic disturbances and the consequent long-term prospective studies. Available studies
increase in the long-term risk of T2D indicate are mostly too small to detect differences in event
that PCOS should be considered a general health rates, and none have shown an evident increase
problem rather than just a reproductive syndrome. in cardiovascular events.76-79 Therefore, the focus
Most investigators found that at least one half of has been on risk factors of cardiovascular disease
PCOS women are obese.8 The prevalence of obesity although these may not necessarily equate with
in PCOS varies widely with the population studied, events or mortality. Studies have found that women
similar to the wide variability in prevalence of obesity with PCOS have an increased carotid intima media
in the general population. thickness and coronary artery calcification, the
Insulin resistance occurs in 60% to 80% of two major surrogate markers for atherosclerotic
women with PCOS, and 95% of obese women cardiovascular disease.80-82 Serum concentrations
with PCOS. The risk of T2D is increased in PCOS, of C-reactive protein, a biochemical predictor of
particularly in women with a first-degree relative cardiovascular disease, also appear to be commonly
with T2D.65 In a systematic review, it was estimated elevated in women with PCOS.83
that the prevalence of impaired glucose tolerance
and T2D was as high as 31% to 35%, and 7.5% to 20%, Patient evaluation
respectively, in women with PCOS by their fourth
decade, and the risks were significantly higher at all Clinical features
ages and all weights even in young or lean subjects The history-taking should include detailed inquiry
with PCOS.66,67 In Hong Kong, the prevalence of T2D about growth and sexual development, menstrual
under 35 years old is 0.6% in the general population, pattern, reproductive history, medical and drug
but 7.5% in women with PCOS.68 history, symptoms of androgen excess, co-existing
Dyslipidaemia is the most common metabolic cardiovascular risk factors such as tobacco and
abnormality in PCOS. Most studies of women alcohol use, and family history. Drug history is
with PCOS have demonstrated low high-density important as a history or current use of sodium
lipoprotein cholesterol and high triglyceride valproate has been shown to be associated with
concentrations, consistent with their insulin PCOS.
resistance, as well as an increase in low-density During the physical examination, it is essential
lipoprotein cholesterol.69-71 to search for signs of androgen excess (hirsutism,
Metabolic syndrome, characterised by a cluster acne, androgenic alopecia) and insulin resistance
of cardiometabolic risk factors associated with in- (acanthosis nigricans). Modified Ferriman-Gallwey
sulin resistance, is a disease with a large health impact scoring is the method generally used to evaluate
as it confers a 5-fold increase in risk of T2D and a clinical hirsutism, but is affected by subjective
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 627
# Yau et al #
variability and cosmetic treatments. It has been exclude late-onset CAH and the 1-mg overnight
suggested that in East Asian patients, a lower cut-off dexamethasone suppression test to exclude
of the modified Ferriman-Gallwey score (of 3) Cushing’s syndrome. It is sometimes noted that
should be used instead of the usual cut-off of 8.16,19 women with PCOS have mildly elevated prolactin.20
As cosmetic hair removal is common in many Asian If the level of 17-hydroxyprogesterone is borderline
countries, evaluation of hirsutism should always elevated, a short synacthen test with measurement
include enquiry about any previous hair-removal of 17-hydroxyprogesterone may be indicated to
procedures. Assessment of blood pressure, BMI, exclude late-onset CAH.19
and waist circumference is also essential. Features Assessment of cardiovascular risk factors
of virilisation, Cushing’s syndrome, and thyroid includes an oral glucose tolerance test (OGTT)
dysfunction should also be looked for and excluded.19 and fasting lipid profiles. Fasting glucose, although
more convenient, has been shown to underestimate
Biochemical features diabetes prevalence and cardiovascular risk when
Laboratory measurements should include tests compared with OGTT, particularly in obese subjects.
to achieve the diagnosis, exclude other endocrine Measuring fasting glucose alone is therefore
problems, and evaluate cardiovascular risk factors. inadequate for the assessment of dysglycaemia in
In someone with clinical signs of hyperandrogenism, women with PCOS.84 Patients with normal glucose
one could argue that biochemical testing is not tolerance should be re-screened at least once every 2
necessary according to current diagnostic criteria. years, or more frequently if additional risk factors are
Most expert groups, however, suggest measuring identified. Patients with impaired glucose tolerance
total testosterone concentration in women who should be screened annually for development of
present with hirsutism. Women with PCOS mostly T2D.
have high-normal or borderline elevated levels of
testosterone. Ultrasound features
Elevated total testosterone is the most direct The use of ultrasound in the diagnosis of PCOS
evidence for androgen excess, but it is important must be tempered by an awareness of the broad
to note that most assays are relatively inaccurate at spectrum of women with ultrasonographic findings
the lower levels present in females, and use of mass characteristic of polycystic ovaries.85 If the patient
spectrometry–based assays of total testosterone are has both oligo-ovulation and hyperandrogenism,
more accurate and preferred.9 Measurement of free a transvaginal ultrasound to document polycystic
testosterone is a more sensitive test, but commer- ovaries is not necessary according to the Rotterdam
cially available free testosterone assays are often criteria. In women who are ready to conceive,
unreliable. The free testosterone index, calculated ultrasound can be used to monitor and document
by total testosterone divided by SHBG, is considered ovulation.
more reliable but is not routinely performed due to The ultrasound criteria in the diagnosis of PCOS
the high cost of measuring SHBG.9 Serum LH and have evolved since the first ultrasound description of
FSH levels should be measured at the early follicular polycystic ovaries in 1986.8 The Rotterdam criteria
phase of the menstrual cycle. Ovulatory assessment described polycystic ovaries as the presence of
such as mid-luteal progesterone measurement is ≥12 follicles in each ovary measuring 2 to 9 mm in
sometimes required in patients seeking infertility diameter and/or increased ovarian volume of >10 mL.
treatment. In rare instances where there are rapidly One ovary fulfilling this definition is sufficient to
progressive features of hyperandrogenism, virilising define polycystic ovaries. More recently, it has
symptoms, or markedly elevated androgen levels been proposed that if newer technology such as
(such as a serum testosterone >5 nmol/L), additional ultrasound machines with transducer frequency
investigations to exclude an androgen-secreting of ≥8 MHz are available, then raising the follicle
tumour may be indicated, including checking cortisol, number per ovary to 25 for diagnosing PCOS would
dehydroepiandrosterone sulfate, and imaging of the be more specific.86
adrenal glands and ovaries. As mentioned earlier, Ultrasonography is operator-dependent
AMH is implicated in the pathogenesis of PCOS, and and requires expertise. Transvaginal ultrasound
recent studies have highlighted its potential utility in is the method of choice, but is practically difficult
the diagnosis of women with PCOS,16 although no in patients without previous sexual experience.
diagnostic cut-off value has been defined yet due to Transrectal ultrasound examination is an alternative
the heterogeneity between the different AMH assay in women where transvaginal scan is not possible.
methods. Transabdominal ultrasound has poorer resolution,
Blood tests to exclude other endocrine especially in obese subjects. Recent research suggests
problems include thyroid function tests, prolactin, that ultrasound might be useful to supplement the
or tests to exclude other underlying causes of excess diagnosis in the event of ovulatory disturbance
androgens, including 17-hydroxyprogesterone to without hyperandrogenism.12,86,87
628 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
Treatment approach Management of hyperandrogenism
The management of women with polycystic ovary As highlighted earlier, administration of an oestrogen-
varies according to the main symptoms and primary containing oral contraceptive has beneficial effects
problem experienced by the patient. The particular on hyperandrogenism. Furthermore, the oral
needs of the patient may change according to different contraceptive pill containing the anti-androgenic
stages of the life course, from adolescence through progestagen cyproterone acetate, administered
to reproductive age.88 Hence management should in cyclical doses, or drospirenone-containing
involve a multidisciplinary approach involving COC might be beneficial for hirsutism.16 The
paediatricians, gynaecologists, endocrinologists, use of cyproterone-containing pills to alleviate
family physicians, dietitians, clinical psychologists, hyperandrogenic symptoms should ideally be
and surgeons, as appropriate.84 limited to short-term use and discontinued 3 to 4
months after symptom resolution due to higher
Management of menstrual irregularity thromboembolic risk than the first-line COC
pills.94 Other anti-androgens, such as finasteride,
Menstrual irregularity is one of the most common
are sometimes used in severe cases of hirsutism,
presenting symptoms of patients with PCOS, and
although again patients need to ensure they avoid
often reflects underlying ovarian dysfunction and
conceiving whilst on anti-androgenic drugs.
anovulation. Chronic anovulation and secondary
In most circumstances, women may elect
amenorrhoea can be associated with endometrial
to use cosmetic measures to treat the clinical
hyperplasia and increased risk of endometrial
manifestations of hyperandrogenism. Different
carcinoma, along with other complications
cosmetic approaches for hair removal—including
associated with amenorrhoea including osteo-
shaving, waxing, and electrolysis—have variable
porosis. Overweight women with PCOS should be
efficacy and duration of effects. Laser therapy in the
encouraged to lose weight; as low as a 5% reduction
form of photoepilation represents a more permanent
in body weight is associated with improvement in
solution but is also more costly.4 Other options for
amenorrhoea.88-90 Previous studies have highlighted
treatment of hirsutism due to hyperandrogenism
that a lifestyle modification programme is associated
include use of topical eflornithine that may help
with improvement in menses, hirsutism, biochemical
reduce excess facial hair.
hyperandrogenism, and insulin resistance.90,91
Progestagens can be administered both as a
diagnostic test to induce progesterone withdrawal, as Management of anovulatory infertility
well as to treat amenorrhoea. Cyclical progestagens, The presence of anovulatory infertility can be
preferably given 12 to 14 days per month, can be investigated by measurement of progesterone in the
used to ensure regular withdrawal bleeding to avoid mid-luteal phase of the menstrual cycle (eg day 21
endometrial hyperplasia, and are associated with of a 28-day cycle, or day 28 of a 35-day cycle), and
less-adverse cardiometabolic effects than combined can help to establish the presence of anovulation.
oestradiol-progestagen pills. Periodic short courses The monitoring of basal body temperature to
of progestogen (2-3 monthly) are an alternative confirm ovulation does not predict ovulation
option. reliably, and is no longer recommended.95 In patients
The use of the combined oral contraceptive with anovulatory infertility, clomiphene treatment
(COC) pill, with its beneficial effects on suppressing is usually considered the first-line treatment.
excess androgen and its manifestations, has been Clomiphene should be started at a low dose (eg 50
a commonly used and convenient treatment mg daily for 5 days per cycle) and gradually increased
for amenorrhoea, with the added benefit of until the lowest effective dose that achieves ovulation
providing contraception. In women with PCOS, is reached, but this requires close monitoring,
COC formulations containing less androgenic especially for the potential side-effects of multiple
progestagens are preferred. Nonetheless, there has pregnancy and ovarian hyperstimulation. Treatment
been some debate about whether the use of COC can be repeated if unsuccessful, but the majority of
may cause exacerbation of cardiometabolic risk.92 patients who respond usually do so within the first
Contra-indications to use of a COC include heavy three cycles.4,96 The highest recommended dose
smokers aged ≥35 years, those with hypertension or for clomiphene is 150 mg, and if the woman still
established cardiac disease, and those with multiple does not respond, second-line treatment should be
cardiovascular risk factors.93 Nevertheless, current considered.
recommendations suggest that this is a useful Metformin has beneficial effects on anovu-
alternative, although clinicians should monitor for lation. In a systematic review and meta-analysis,
changes in body weight, blood pressure, lipid profile metformin was found to be associated with increased
as well as dysglycaemia if patients are prescribed success at inducing ovulation.97 Doses vary in clinical
COC, especially if the patient is overweight. trials from 1 g daily to higher doses. In a multicentre
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 629
# Yau et al #
randomised controlled trial, therapy-naїve PCOS Management of cardiometabolic risk
women who received metformin had a significantly Women with PCOS are at substantially increased
lower live birth rate than women who conceived cardiometabolic risk, and therefore should
through clomiphene alone, or were treated with a undergo periodic evaluation of associated risk
combination of clomiphene and metformin.98 The factors.4 Overweight women with PCOS should
use of metformin as a co-treatment with clomiphene undergo comprehensive evaluation by a dietitian,
has been shown to improve ovulation in women and be encouraged to lose weight. Weight loss
with clomiphene-resistant PCOS.99 Metformin of approximately 5% is already associated with
is in general stopped after successful conception, improved metabolic parameters as well as
although some advocate continued use during the reproductive outcome. Even among women with
first trimester to reduce the risk of spontaneous normal BMI, those with PCOS appear to have
miscarriage. This is still an area of controversy, and increased visceral adiposity that contributes to the
the pros and cons of continuing metformin should endogenous insulin resistance, and is correlated with
be carefully discussed. Metformin is known to cross metabolic parameters, fatty liver as well as carotid
the placenta but it has also been shown to be a useful intimal-medial thickness.103
treatment for gestational diabetes. In addition to lifestyle measures, women
Aromatase inhibitors reduce circulating should be screened for glucose intolerance by an
oestrogen levels, lead to a rise in pituitary FSH, and OGTT. Screening using fasting glucose alone is
have previously shown beneficial effects in a meta- inadequate in this high-risk population.4 Presence of
analysis. Letrozole, an aromatase inhibitor, was impaired glucose tolerance may warrant treatment
found to be superior to clomiphene in achieving live with metformin given the multiple metabolic and
births in a randomised clinical trial.100 reproductive benefits, regardless of whether there
Daily injections of exogenous gonadotropins, is clinical evidence of insulin resistance. Overt
including recombinant FSH or menopausal diabetes should be treated using an appropriate
gonadotropin, have been found to improve ovulation combination of dietary treatment, metformin, other
induction among women who did not respond to oral glucose-lowering agents, and in some cases,
other treatments. This treatment requires careful insulin. The choice of agent should depend on the
monitoring, and should be used with a ‘chronic low- underlying pathophysiology (eg whether obesity
dose step-up’ approach as outlined by the ESHRE/ is present), but also take into account the fertility
ASRM to avoid multiple pregnancies or ovarian wishes and plans of the patient. Metformin in
hyperstimulation syndrome.96,101 combination with lifestyle intervention has been
found to be associated with greater reduction in
Ovarian surgery/drilling/laparoscopic ovarian BMI compared with lifestyle intervention alone.104
diathermy Several studies have demonstrated the efficacy of
Surgical procedures such as ovarian wedge resection thiazolidinediones in improving metabolic para-
or ovarian drilling by diathermy or laser lead to a meters as well as menses and hyperandrogenism
decreased number of antral follicles, reduced ovarian in women with PCOS. Due to possible adverse
androgen production, and improved ovulation.16 effects, however, this class of agent is currently not
Ovarian wedge resection is no longer performed recommended for treatment of insulin resistance
due to the higher extent of adhesion formation and among women with PCOS.4
ovarian tissue damage. Ovarian drilling has been Treatment of hypertension likewise should
used as an alternative to exogenous gonadotropins take into account the fertility wishes of the patient.
for treatment of anovulatory infertility, with Screening for other secondary causes of young-
similar success rates. The main limitations onset hypertension may be necessary, especially
include the potential for formation of adhesions, if atypical features such as proteinuria are present.
and reduced ovarian reserve. In a retrospective Preferred anti-hypertensive agents in women
analysis of Chinese women with PCOS treated by contemplating pregnancy would be the older agents
laser diathermy, spontaneous ovulation rates and such as methyldopa. It is notable that women
cumulative pregnancy rates were similar regardless with pre-existing hypertension are more likely
of the presence or absence of metabolic syndrome.102 to develop hypertension-related complications
during pregnancy, and therefore require more strict
surveillance during pregnancy. Hyperlipidaemia can
Assisted reproductive procedures
be managed using dietary measures, and in some
In women who fail second-line treatment such as cases, lipid-lowering agents such as HMG CoA
metformin, ovarian drilling or ovarian stimulation (3-hydroxy-3-methylglutaryl coenzyme A) reductase
with gonadotropins, third-line treatment such as inhibitors. If there are plans for pregnancy, drug
intrauterine insemination or in-vitro fertilisation treatment with lipid-lowering treatment should be
can be considered.17 withheld.
630 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
Psychological distress, anxiety, and depression Acknowledgement
are common among women with PCOS, and may
be linked to some of the skin complications such as RCW Ma acknowledges support from the Research
hirsutism and acne or presence of menstrual and Grants Council General Research Fund (Ref.
fertility problems; all these impact on psychological 14110415).
well-being. Clinicians need to have a high level of
awareness and screen for these symptoms when Declaration
appropriate and offer the necessary referrals for All authors have disclosed no conflicts of interest.
psychological support. Sleep-disordered breathing
including obstructive sleep apnoea is also common, References
impacts sleep quality, and can exacerbate both 1. Stein IF, Leventhal ML. Amenorrhea associated with
mood problems as well as cardiometabolic risk. It bilateral polycystic ovaries. Am J Obstet Gynecol
should be screened for and managed accordingly. 1935;29:181-91.
In those with marked obesity, bariatric surgery 2. March WA, Moore VM, Willson KJ, Phillips DI, Norman
is an option to address obesity and associated RJ, Davies MJ. The prevalence of polycystic ovary syndrome
in a community sample assessed under contrasting
metabolic abnormalities. Interestingly, a systematic
diagnostic criteria. Hum Reprod 2010;25:544-51.
review including 13 primary studies found that the
3. Chen X, Yang D, Mo Y, Li L, Chen Y, Huang Y. Prevalence
incidence of PCOS was reduced from 45.6% to 7.1% of polycystic ovary syndrome in unselected women
after bariatric surgery.105 from southern China. Eur J Obstet Gynecol Reprod Biol
The screening and management of metabolic 2008;139:59-64.
abnormalities is particularly relevant in those 4. Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis
women with PCOS who are planning a pregnancy or and treatment of polycystic ovary syndrome: an Endocrine
undergoing fertility treatment. Women with PCOS Society clinical practice guideline. J Clin Endocrinol Metab
are at increased risk of different complications 2013;98:4565-92.
including gestational diabetes and pre-eclampsia. 5. Gibson-Helm M, Teede H, Dunaif A, Dokras A. Delayed
Undiagnosed gestational diabetes/maternal diagnosis and a lack of information associated with
dissatisfaction in women with polycystic ovary syndrome.
hyperglycaemia or poorly controlled blood pressure
J Clin Endocrinol Metab 2017;102:604-12.
all contribute to poorer pregnancy outcome among
6. Zawadski J, Dunaif A. Diagnostic criteria for polycystic
women with PCOS. Optimal management before ovary syndrome: towards a rational approach. In: Dunaif A,
pregnancy and intrapartum can help to minimise the Givens JR, Haseltine FP, Merriam GR, editors. Polycystic
risk of these pregnancy complications. ovary syndrome. Boston: Blackwell Scientific Publications;
1992: 377-84.
Conclusions 7. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus
Workshop Group. Revised 2003 consensus on diagnostic
Polycystic ovary syndrome is a multi-faceted criteria and long-term health risks related to polycystic
syndrome that is becoming increasingly recognised, ovary syndrome. Fertil Steril 2004;81:19-25.
and is an important contributor to multiple medical 8. Azziz R, Carmina E, Dewailly D, et al. The Androgen
and reproductive problems. As illustrated in Excess and PCOS Society criteria for the polycystic ovary
this review, given the multiple reproductive and syndrome: the complete task force report. Fertil Steril
metabolic complications associated with PCOS, 2009;91:456-88.
9. Rosner W, Auchus RJ, Azziz R, Sluss PM, Raff H. Position
patients may seek medical attention via a variety
statement: utility, limitations, and pitfalls in measuring
of different channels, and may present to clinicians
testosterone: an Endocrine Society position statement. J
through different disciplines. Clinicians therefore Clin Endocrinol Metab 2007;92:405-13.
need to recognise the multi-faceted nature of this 10. Evidence-based Methodology Workshop on Polycystic
complex disorder and be aware of the associated Ovary Syndrome (PCOS). December 3-5, 2012. Available
complications. Diagnostic criteria are still evolving, from: https://www.nichd.nih.gov/about/meetings/2012/
although currently the Rotterdam criteria remain the Pages/120512.aspx. Accessed 10 Jul 2017.
most widely accepted. Given the burden of metabolic 11. Lam PM, Ma RC, Cheung LP, Chow CC, Chan JC, Haines
complications associated with the disorder, there has CJ. Polycystic ovarian syndrome in Hong Kong Chinese
been much recent discussion regarding the potential women: patient characteristics and diagnostic criteria.
need to rename the syndrome to better highlight its Hong Kong Med J 2005;11:336-41.
12. Boyle JA, Teede HJ. PCOS: Refining diagnostic features in
metabolic consequences, in addition to the known
PCOS to optimize health outcomes. Nat Rev Endocrinol
reproductive features. The long-term risks of the
2016;12:630-1.
different complications are still not clearly defined, 13. Rojas J, Chávez M, Olivar L, et al. Polycystic ovary
given the scarcity of well-conducted prospective syndrome, insulin resistance, and obesity: navigating
studies. These limitations in our current knowledge the pathophysiologic labyrinth. Int J Reprod Med
highlight the need to follow-up this group of high- 2014;2014:719050.
risk women. 14. Cheung LP. Polycystic ovary syndrome: not only a
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 631
# Yau et al #
gynaecological disease. J Paediatr Obstet Gynaecol response to adrenocorticotropin in hyperandrogenic
2008(May/Jun):125-31. women: apparent relative impairment of 17,20-lyase
15. Diamanti-Kandarakis E, Piperi C. Genetics of polycystic activity. J Clin Endocrinol Metab 1996;81:881-6.
ovary syndrome: searching for the way out of the labyrinth. 34. Yki-Järvinen H, Mäkimattila S, Utriainen T, Rutanen
Hum Reprod Update 2005;11:631-43. EM. Portal insulin concentrations rather than insulin
16. Azziz R, Carmina E, Chen Z, et al. Polycystic ovary sensitivity regulate serum sex hormone-binding globulin
syndrome. Nat Rev Dis Primers 2016;2:16057. and insulin-like growth factor binding protein 1 in vivo. J
17. Goodarzi MO, Dumesic DA, Chazenbalk G, Azziz R. Clin Endocrinol Metab 1995;80:3227-32.
Polycystic ovary syndrome: etiology, pathogenesis and 35. Poretsky L, Cataldo NA, Rosenwaks Z, Giudice LC. The
diagnosis. Nat Rev Endocrinol 2011;7:219-31. insulin-related ovarian regulatory system in health and
18. Azziz R, Carmina E, Dewailly D, et al. Positions statement: disease. Endocr Rev 1999;20:535-82.
criteria for defining polycystic ovary syndrome as a 36. Gambineri A, Patton L, Altieri P, et al. Polycystic ovary
predominantly hyperandrogenic syndrome: an Androgen syndrome is a risk factor for type 2 diabetes: results from a
Excess Society guideline. J Clin Endocrinol Metab long-term prospective study. Diabetes 2012;61:2369-74.
2006;91:4237-45. 37. Bremer AA, Miller WL. The serine phosphorylation
19. McCartney CR, Marshall JC. Clinical practice. Polycystic hypothesis of polycystic ovary syndrome: a unifying
ovary syndrome. N Engl J Med 2016;375:54-64. mechanism for hyperandrogenemia and insulin resistance.
20. Franks S. Polycystic ovary syndrome. N Engl J Med Fertil Steril 2008;89:1039-48.
1995;333:853-61. 38. Corbould A, Kim YB, Youngren JF, et al. Insulin resistance
21. Agarwal SK, Judd HL, Magoffin DA. A mechanism for the in the skeletal muscle of women with PCOS involves
suppression of estrogen production in polycystic ovary intrinsic and acquired defects in insulin signaling. Am J
syndrome. J Clin Endocrinol Metab 1996;81:3686-91. Physiol Endocrinol Metab 2005;288:E1047-54.
22. Jakimiuk AJ, Weitsman SR, Magoffin DA. 5alpha-reductase 39. Dunaif A, Segal KR, Futterweit W, Dobrjansky A. Profound
activity in women with polycystic ovary syndrome. J Clin peripheral insulin resistance, independent of obesity, in
Endocrinol Metab 1999;84:2414-8. polycystic ovary syndrome. Diabetes 1989;38:1165-74.
23. Moghetti P, Castello R, Negri C, et al. Metformin effects 40. Stepto NK, Cassar S, Joham AE, et al. Women with
on clinical features, endocrine and metabolic profiles, polycystic ovary syndrome have intrinsic insulin resistance
and insulin sensitivity in polycystic ovary syndrome: a on euglycaemic-hyperinsulaemic clamp. Hum Reprod
randomized, double-blind, placebo-controlled 6-month 2013;28:777-84.
trial, followed by open, long-term clinical evaluation. J Clin 41. Legro RS. Diabetes prevalence and risk factors in
Endocrinol Metab 2000;85:139-46. polycystic ovary syndrome. Obstet Gynecol Clin North
24. Bergh C, Carlsson B, Olsson JH, Selleskog U, Hillensjö T. Am 2001;28:99-109.
Regulation of androgen production in cultured human 42. Dunaif A, Finegood DT. Beta-cell dysfunction independent
thecal cells by insulin-like growth factor I and insulin. of obesity and glucose intolerance in the polycystic ovary
Fertil Steril 1993;59:323-31. syndrome. J Clin Endocrinol Metab 1996;81:942-7.
25. Balen AH, Conway G, Homburg R, Legro R. Polycystic 43. Ehrmann DA, Kasza K, Azziz R, Legro RS, Ghazzi MN;
ovary syndrome: A guide to clinical management. UK: PCOS/Troglitazone Study Group. Effects of race and
Taylor & Francis; 2006. family history of type 2 diabetes on metabolic status of
26. Franks S, Gilling-Smith C, Watson H, Willis D. Insulin women with polycystic ovary syndrome. J Clin Endocrinol
action in the normal and polycystic ovary. Endocrinol Metab 2005;90:66-71.
Metab Clin North Am 1999;28:361-78. 44. Dunaif A, Wu X, Lee A, Diamanti-Kandarakis E. Defects
27. Knight PG, Glister C. Local roles of TGF-beta superfamily in insulin receptor signaling in vivo in the polycystic
members in the control of ovarian follicle development. ovary syndrome (PCOS). Am J Physiol Endocrinol Metab
Anim Reprod Sci 2003;78:165-83. 2001;281:E392-9.
28. Seifer DB, MacLaughlin DT, Cuckle HS. Serum mullerian- 45. Ciaraldi TP, Aroda V, Mudaliar S, Chang RJ, Henry RR.
inhibiting substance in Down’s syndrome pregnancies. Polycystic ovary syndrome is associated with tissue-
Hum Reprod 2007;22:1017-20. specific differences in insulin resistance. J Clin Endocrinol
29. Visser JA, de Jong FH, Laven JS, Themmen AP. Anti- Metab 2009;94:157-63.
Müllerian hormone: a new marker for ovarian function. 46. Ciaraldi TP. Molecular defects of insulin action in the
Reproduction 2006;131:1-9. polycystic ovary syndrome: possible tissue specificity. J
30. Pellatt L, Hanna L, Brincat M, et al. Granulosa cell Pediatr Endocrinol Metab 2000;13 Suppl 5:1291-3.
production of anti-Müllerian hormone is increased in 47. Ibáñez L, Sebastiani G, Diaz M, Gómez-Roig MD, Lopez-
polycystic ovaries. J Clin Endocrinol Metab 2007;92:240-5. Bermejo A, de Zegher F. Low body adiposity and high
31. Dunaif A. Insulin resistance and the polycystic ovary leptinemia in breast-fed infants born small-for-gestational-
syndrome: mechanism and implications for pathogenesis. age. J Pediatr 2010;156:145-7.
Endocr Rev 1997;18:774-800. 48. Virtue S, Vidal-Puig A. It’s not how fat you are, it’s what you
32. Diamanti-Kandarakis E, Argyrakopoulou G, Economou F, do with it that counts. PLoS Biol 2008;6:e237.
Kandaraki E, Koutsilieris M. Defects in insulin signaling 49. Virtue S, Vidal-Puig A. Adipose tissue expandability,
pathways in ovarian steroidogenesis and other tissues in lipotoxicity and the metabolic syndrome—an allostatic
polycystic ovary syndrome (PCOS). J Steroid Biochem Mol perspective. Biochim Biophys Acta 2010;1801:338-49.
Biol 2008;109:242-6. 50. Chazenbalk G, Trivax BS, Yildiz BO, et al. Regulation of
33. Moghetti P, Castello R, Negri C, et al. Insulin infusion adiponectin secretion by adipocytes in the polycystic ovary
amplifies 17 alpha-hydroxycorticosteroid intermediates syndrome: role of tumor necrosis factor-{alpha}. J Clin
632 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
# Polycystic ovary syndrome #
Endocrinol Metab 2010;95:935-42. SF. Risk of T2DM and impaired fasting glucose among
51. Barber TM, Franks S. Adipocyte biology in polycystic PCOS subjects: results of an 8-year follow-up. Curr Diab
ovary syndrome. Mol Cell Endocrinol 2013;373:68-76. Rep 2006;6:77-83.
52. Padmanabhan V, Manikkam M, Recabarren S, Foster D. 68. Cheung LP, Ma RC, Lam PM, et al. Cardiovascular risks and
Prenatal testosterone excess programs reproductive and metabolic syndrome in Hong Kong Chinese women with
metabolic dysfunction in the female. Mol Cell Endocrinol polycystic ovary syndrome. Hum Reprod 2008;23:1431-8.
2006;246:165-74. 69. Berneis K, Rizzo M, Lazzarini V, Fruzzetti F, Carmina
53. Dumesic DA, Schramm RD, Abbott DH. Early origins of E. Atherogenic lipoprotein phenotype and low-density
polycystic ovary syndrome. Reprod Fertil Dev 2005;17:349- lipoproteins size and subclasses in women with polycystic
60. ovary syndrome. J Clin Endocrinol Metab 2007;92:186-
54. Legro RS, Bentley-Lewis R, Driscoll D, Wang SC, Dunaif A. 9.
Insulin resistance in the sisters of women with polycystic 70. Phelan N, O’Connor A, Kyaw-Tun T, et al. Lipoprotein
ovary syndrome: association with hyperandrogenemia subclass patterns in women with polycystic ovary syndrome
rather than menstrual irregularity. J Clin Endocrinol (PCOS) compared with equally insulin-resistant women
Metab 2002;87:2128-33. without PCOS. J Clin Endocrinol Metab 2010;95:3933-9.
55. Hickey M, Sloboda DM, Atkinson HC, et al. The relationship 71. Valkenburg O, Steegers-Theunissen RP, Smedts HP, et al.
between maternal and umbilical cord androgen levels and A more atherogenic serum lipoprotein profile is present
polycystic ovary syndrome in adolescence: a prospective in women with polycystic ovary syndrome: a case-control
cohort study. J Clin Endocrinol Metab 2009;94:3714-20. study. J Clin Endocrinol Metab 2008;93:470-6.
56. Dumesic DA, Oberfield SE, Stener-Victorin E, Marshall JC, 72. Isomaa B, Almgren P, Tuomi T, et al. Cardiovascular
Laven JS, Legro RS. Scientific statement on the diagnostic morbidity and mortality associated with the metabolic
criteria, epidemiology, pathophysiology, and molecular syndrome. Diabetes Care 2001;24:683-9.
genetics of polycystic ovary syndrome. Endocr Rev 73. Weerakiet S, Bunnag P, Phakdeekitcharoen B, et al.
2015;36:487-525. Prevalence of the metabolic syndrome in Asian women
57. Hayes MG, Urbanek M, Ehrmann DA, et al. Genome- with polycystic ovary syndrome: using the International
wide association of polycystic ovary syndrome implicates Diabetes Federation criteria. Gynecol Endocrinol
alterations in gonadotropin secretion in European ancestry 2007;23:153-60.
populations. Nat Commun 2015;6:7502. 74. Vgontzas AN, Legro RS, Bixler EO, Grayev A, Kales A,
58. Boomsma CM, Eijkemans MJ, Hughes EG, Visser GH, Chrousos GP. Polycystic ovary syndrome is associated
Fauser BC, Macklon NS. A meta-analysis of pregnancy with obstructive sleep apnea and daytime sleepiness: role
outcomes in women with polycystic ovary syndrome. Hum of insulin resistance. J Clin Endocrinol Metab 2001;86:517-
Reprod Update 2006;12:673-83. 20.
59. Weerakiet S, Srisombut C, Rojanasakul A, Panburana P, 75. Gopal M, Duntley S, Uhles M, Attarian H. The role of
Thakkinstian A, Herabutya Y. Prevalence of gestational obesity in the increased prevalence of obstructive sleep
diabetes mellitus and pregnancy outcomes in Asian women apnea syndrome in patients with polycystic ovarian
with polycystic ovary syndrome. Gynecol Endocrinol syndrome. Sleep Med 2002;3:401-4.
2004;19:134-40. 76. Wild S, Pierpoint T, McKeigue P, Jacobs H. Cardiovascular
60. Qin JZ, Pang LH, Li MJ, Fan XJ, Huang RD, Chen HY. disease in women with polycystic ovary syndrome at
Obstetric complications in women with polycystic ovary long-term follow-up: a retrospective cohort study. Clin
syndrome: a systematic review and meta-analysis. Reprod Endocrinol (Oxf ) 2000;52:595-600.
Biol Endocrinol 2013;11:56. 77. Lo JC, Feigenbaum SL, Yang J, Pressman AR, Selby JV, Go
61. Chittenden BG, Fullerton G, Maheshwari A, Bhattacharya AS. Epidemiology and adverse cardiovascular risk profile
S. Polycystic ovary syndrome and the risk of gynaecological of diagnosed polycystic ovary syndrome. J Clin Endocrinol
cancer: a systematic review. Reprod Biomed Online Metab 2006;91:1357-63.
2009;19:398-405. 78. Cibula D, Cifkova R, Fanta M, Poledne R, Zivny J, Skibova
62. Haoula Z, Salman M, Atiomo W. Evaluating the association J. Increased risk of non-insulin dependent diabetes
between endometrial cancer and polycystic ovary mellitus, arterial hypertension and coronary artery disease
syndrome. Hum Reprod 2012;27:1327-31. in perimenopausal women with a history of the polycystic
63. Timmermans A, Opmeer BC, Khan KS, et al. Endometrial ovary syndrome. Hum Reprod 2000;15:785-9.
thickness measurement for detecting endometrial cancer 79. Schmidt J, Landin-Wilhelmsen K, Brännström M,
in women with postmenopausal bleeding: a systematic Dahlgren E. Cardiovascular disease and risk factors in
review and meta-analysis. Obstet Gynecol 2010;116:160-7. PCOS women of postmenopausal age: a 21-year controlled
64. Sartor BM, Dickey RP. Polycystic ovarian syndrome and follow-up study. J Clin Endocrinol Metab 2011;96:3794-
the metabolic syndrome. Am J Med Sci 2005;330:336-42. 803.
65. Colilla S, Cox NJ, Ehrmann DA. Heritability of insulin 80. Shroff R, Kerchner A, Maifeld M, Van Beek EJ, Jagasia
secretion and insulin action in women with polycystic D, Dokras A. Young obese women with polycystic ovary
ovary syndrome and their first degree relatives. J Clin syndrome have evidence of early coronary atherosclerosis.
Endocrinol Metab 2001;86:2027-31. J Clin Endocrinol Metab 2007;92:4609-14.
66. Legro RS, Gnatuk CL, Kunselman AR, Dunaif A. Changes 81. Luque-Ramirez M, Mendieta-Azcona C, Alvarez-Blasco F,
in glucose tolerance over time in women with polycystic Escobar-Morreale HF. Androgen excess is associated with
ovary syndrome: a controlled study. J Clin Endocrinol the increased carotid intima-media thickness observed
Metab 2005;90:3236-42. in young women with polycystic ovary syndrome. Hum
67. Boudreaux MY, Talbott EO, Kip KE, Brooks MM, Witchel Reprod 2007;22:3197-203.
Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org 633
# Yau et al #
82. Talbott EO, Zborowski JV, Rager JR, Boudreaux MY, contraceptive use. 2015. Available from: http://apps.who.
Edmundowicz DA, Guzick DS. Evidence for an association int/iris/bitstream/10665/181468/1/9789241549158_eng.
between metabolic cardiovascular syndrome and coronary pdf. Accessed 10 Jul 2017.
and aortic calcification among women with polycystic 94. The Faculty of Sexual and Reproductive Healthcare of the
ovary syndrome. J Clin Endocrinol Metab 2004;89:5454- Royal College of Obstetricians and Gynaecologists (FSRH).
61. FSRH Statement: Venous thromboembolism (VTE) and
83. Boulman N, Levy Y, Leiba R, et al. Increased C-reactive hormonal contraception Nov 2014. Available from: https://
protein levels in the polycystic ovary syndrome: a marker www.fsrh.org/standards-and-guidance/documents/fsr
of cardiovascular disease. J Clin Endocrinol Metab hstatementvteandhormonalcontraception-november/.
2004;89:2160-5. Accessed 10 Jul 2017.
84. Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on 95. National Institute for Health and Care Excellence. Fertility
women’s health aspects of polycystic ovary syndrome problems: assessment and treatment. 20 Feb 2013.
(PCOS): the Amsterdam ESHRE/ASRM-Sponsored Available from: https://www.nice.org.uk/guidance/cg156.
3rd PCOS Consensus Workshop Group. Fertil Steril Accessed 10 Jul 2017.
2012;97:28-38.e25. 96. Jayasena CN, Franks S. The management of patients
85. Johnstone EB, Rosen MP, Neril R, et al. The polycystic with polycystic ovary syndrome. Nat Rev Endocrinol
ovary post-rotterdam: a common, age-dependent finding 2014;10:624-36.
in ovulatory women without metabolic significance. J Clin 97. Lord JM, Flight IH, Norman RJ. Metformin in polycystic
Endocrinol Metab 2010;95:4965-72. ovary syndrome: systematic review and meta-analysis.
86. Dewailly D, Lujan ME, Carmina E, et al. Definition and BMJ 2003;327:951-3.
significance of polycystic ovarian morphology: a task force 98. Legro RS, Barnhart HX, Schlaff WD, et al. Clomiphene,
report from the Androgen Excess and Polycystic Ovary metformin, or both for infertility in the polycystic ovary
Syndrome Society. Hum Reprod Update 2014;20:334-52. syndrome. N Engl J Med 2007;356:551-66.
87. Quinn MM, Kao CN, Ahmad A, et al. Raising threshold 99. Moll E, van der Veen F, van Wely M. The role of metformin
for diagnosis of polycystic ovary syndrome excludes in polycystic ovary syndrome: a systematic review. Hum
population of patients with metabolic risk. Fertil Steril Reprod Update 2007;13:527-37.
2016;106:1244-51. 100. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus
88. Conway G, Dewailly D, Diamanti-Kandarakis E, et al. The clomiphene for infertility in the polycystic ovary syndrome.
polycystic ovary syndrome: a position statement from N Engl J Med 2014;371:119-29.
the European Society of Endocrinology. Eur J Endocrinol 101. Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus
2014;171:P1-29. Workshop Group. Consensus on infertility treatment
89. Moran LJ, Noakes M, Clifton PM, Tomlinson L, Galletly C, related to polycystic ovary syndrome. Hum Reprod
Norman RJ. Dietary composition in restoring reproductive 2008;23:462-77.
and metabolic physiology in overweight women with 102. Kong GW, Cheung LP, Lok IH. Effects of laparoscopic
polycystic ovary syndrome. J Clin Endocrinol Metab ovarian drilling in treating infertile anovulatory polycystic
2003;88:812-9. ovarian syndrome patients with and without metabolic
90. Moran LJ, Hutchison SK, Norman RJ, Teede HJ. Lifestyle syndrome. Hong Kong Med J 2011;17:5-10.
changes in women with polycystic ovary syndrome. 103. Ma RC, Liu KH, Lam PM, et al. Sonographic measurement
Cochrane Database Syst Rev 2011;(7):CD007506. of mesenteric fat predicts presence of fatty liver among
91. Pasquali R, Gambineri A, Pagotto U. The impact of subjects with polycystic ovary syndrome. J Clin Endocrinol
obesity on reproduction in women with polycystic ovary Metab 2011;96:799-807.
syndrome. BJOG 2006;113:1148-59. 104. Naderpoor N, Shorakae S, de Courten B, Misso ML,
92. Diamanti-Kandarakis E, Baillargeon JP, Iuorno MJ, Moran LJ, Teede HJ. Metformin and lifestyle modification
Jakubowicz DJ, Nestler JE. A modern medical quandary: in polycystic ovary syndrome: systematic review and meta-
polycystic ovary syndrome, insulin resistance, and oral analysis. Hum Reprod Update 2015;21:560-74.
contraceptive pills. J Clin Endocrinol Metab 2003;88:1927- 105. Skubleny D, Switzer NJ, Gill RS, et al. The impact of bariatric
32. surgery on polycystic ovary syndrome: a systematic review
93. World Health Organization. Medical eligibility criteria for and meta-analysis. Obes Surg 2016;26:169-76.
634 Hong Kong Med J ⎥ Volume 23 Number 6 ⎥ December 2017 ⎥ www.hkmj.org
Potrebbero piacerti anche
- Current Aspects of Polycystic Ovary Syndrome A Literature ReviewDocumento5 pagineCurrent Aspects of Polycystic Ovary Syndrome A Literature ReviewlizandrobNessuna valutazione finora
- Seminar: Robert J Norman, Didier Dewailly, Richard S Legro, Theresa E HickeyDocumento13 pagineSeminar: Robert J Norman, Didier Dewailly, Richard S Legro, Theresa E HickeyMédica Consulta ExternaNessuna valutazione finora
- Clinical Presentation and Diagnosis of Polycystic Ovarian SyndromeDocumento9 pagineClinical Presentation and Diagnosis of Polycystic Ovarian SyndromeLia MeivianeNessuna valutazione finora
- Primary and Secondary Prevention of Metabolic and Cardiovascular Comorbidities in Women With Polycystic Ovary SyndromeDocumento8 paginePrimary and Secondary Prevention of Metabolic and Cardiovascular Comorbidities in Women With Polycystic Ovary SyndromeMelisa Viviana Zapata NavarroNessuna valutazione finora
- 3 - Pcos Tog 2017Documento11 pagine3 - Pcos Tog 2017Siti NurfathiniNessuna valutazione finora
- Polycystic Ovary Syndrome 2016 NEJMDocumento11 paginePolycystic Ovary Syndrome 2016 NEJMGabrielaNessuna valutazione finora
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Documento11 pagine6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaNessuna valutazione finora
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyDa EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNessuna valutazione finora
- LECTURE 24 Polycystic Ovary SyndromeDocumento13 pagineLECTURE 24 Polycystic Ovary SyndromeCharisse Angelica MacedaNessuna valutazione finora
- 1 s2.0 S0026049517302743 MainDocumento11 pagine1 s2.0 S0026049517302743 MainTeodora OnofreiNessuna valutazione finora
- Diagnosis and Management of Adoslecent PCOS 2020Documento11 pagineDiagnosis and Management of Adoslecent PCOS 2020Awan AndrawinuNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento13 paginePolycystic Ovary SyndromeLIZARDO CRUZADO DIAZNessuna valutazione finora
- 7 FixDocumento5 pagine7 FixalmubarakhNessuna valutazione finora
- China PCOSDocumento14 pagineChina PCOSMayene ChavezNessuna valutazione finora
- ReviewDocumento13 pagineReviewNelly ElizabethNessuna valutazione finora
- An Update of Genetic BasisDocumento10 pagineAn Update of Genetic BasisHAVIZ YUADNessuna valutazione finora
- AACE/ACE Disease State Clinical ReviewDocumento10 pagineAACE/ACE Disease State Clinical ReviewSanjay NavaleNessuna valutazione finora
- MetforminDocumento14 pagineMetforminnidyaNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento13 paginePolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento11 paginePolycystic Ovary SyndromeViridiana Briseño GarcíaNessuna valutazione finora
- 3.review of Literature PDFDocumento38 pagine3.review of Literature PDFJalajarani AridassNessuna valutazione finora
- Theft of Womanhood - Polycystic Ovarian Syndrome: Role of HomeopathyDocumento11 pagineTheft of Womanhood - Polycystic Ovarian Syndrome: Role of HomeopathyMadhukar KNessuna valutazione finora
- Ovario PoliqDocumento16 pagineOvario PoliqlizethNessuna valutazione finora
- Acog 194Documento15 pagineAcog 194Marco DiestraNessuna valutazione finora
- Endocrinology & Metabolic SyndromeDocumento13 pagineEndocrinology & Metabolic SyndromeMayra PereiraNessuna valutazione finora
- Rajiv Gandhi University of Health Sciences: 20 October 2011Documento8 pagineRajiv Gandhi University of Health Sciences: 20 October 2011Manali JainNessuna valutazione finora
- Kri Edt 2018Documento5 pagineKri Edt 2018Teguh Imana NugrahaNessuna valutazione finora
- Whats New of PcosDocumento9 pagineWhats New of PcosbambangNessuna valutazione finora
- Chapter 27 The Polycystic Ovary SyndromeDocumento4 pagineChapter 27 The Polycystic Ovary Syndromepmj050gpNessuna valutazione finora
- Polycysticovarysyndrome Inadolescents: Selma Feldman Witchel,, Hailey Roumimper,, Sharon OberfieldDocumento16 paginePolycysticovarysyndrome Inadolescents: Selma Feldman Witchel,, Hailey Roumimper,, Sharon OberfieldAgustina S. SelaNessuna valutazione finora
- ARPCKD Bombay J 2012Documento4 pagineARPCKD Bombay J 2012micamica451Nessuna valutazione finora
- Insulin Resistance and PCOS-dr. Hilma Final 11 Juli 2021 FIXDocumento48 pagineInsulin Resistance and PCOS-dr. Hilma Final 11 Juli 2021 FIXputrihealthirezaNessuna valutazione finora
- Fitzgerald 2018Documento7 pagineFitzgerald 2018Derevie Hendryan MoulinaNessuna valutazione finora
- Resistencia InsulinaDocumento13 pagineResistencia InsulinaNutrición MxNessuna valutazione finora
- Clep 6 001 PDFDocumento13 pagineClep 6 001 PDFJaila NatashaNessuna valutazione finora
- GWAS PCOS KoreaDocumento9 pagineGWAS PCOS KoreaedwardNessuna valutazione finora
- Jurnal Pcos InternationalDocumento5 pagineJurnal Pcos InternationalPuput Anistiya Hariani100% (1)
- Jeanes 2017Documento9 pagineJeanes 2017ThormmmNessuna valutazione finora
- Costello 2007Documento10 pagineCostello 2007ThormmmNessuna valutazione finora
- PCOS-Journal Article 2Documento8 paginePCOS-Journal Article 2dinarosman02Nessuna valutazione finora
- Jurnal 7Documento10 pagineJurnal 7Ade Yurga TonaraNessuna valutazione finora
- Polycystic Ovary Syndrome Throughout A Woman's LifeDocumento15 paginePolycystic Ovary Syndrome Throughout A Woman's LifeMDLuchoNessuna valutazione finora
- Metformin in PCOSDocumento5 pagineMetformin in PCOSbalaramNessuna valutazione finora
- GYNE - Polycystic Ovarian Syndrome (PCOS)Documento7 pagineGYNE - Polycystic Ovarian Syndrome (PCOS)Alodia Razon100% (1)
- Jpe 3 E05Documento6 pagineJpe 3 E05amirreza jmNessuna valutazione finora
- ICP AnnalsofhepatologyDocumento4 pagineICP AnnalsofhepatologyArnella HutagalungNessuna valutazione finora
- Association of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian SyndromeDocumento4 pagineAssociation of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian Syndromedoctor wajihaNessuna valutazione finora
- Pregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor RahmanDocumento6 paginePregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor Rahmanmr1998goNessuna valutazione finora
- Rosenfield2015 PDFDocumento27 pagineRosenfield2015 PDFdanilacezaraalinaNessuna valutazione finora
- Case Report: Pregnancy in An Infertile Woman With Polycystic Ovary SyndromeDocumento4 pagineCase Report: Pregnancy in An Infertile Woman With Polycystic Ovary SyndromeEunice PalloganNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento6 paginePolycystic Ovary SyndromealemNessuna valutazione finora
- Female Genomics Infertility and Overall Health Joshi 2017Documento8 pagineFemale Genomics Infertility and Overall Health Joshi 2017Orlando CuellarNessuna valutazione finora
- Survey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiaDocumento9 pagineSurvey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiayooyoNessuna valutazione finora
- Survey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiaDocumento9 pagineSurvey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiayooyoNessuna valutazione finora
- Jama Huddleston 2022 It 210031 1641843898.23442Documento2 pagineJama Huddleston 2022 It 210031 1641843898.23442Davi LeocadioNessuna valutazione finora
- Hyperemesis Gravidarum 2019 NatureDocumento17 pagineHyperemesis Gravidarum 2019 NatureResidentes GinecologíaNessuna valutazione finora
- Abdominal Adiposity and The Polycystic Ovary SyndromeDocumento7 pagineAbdominal Adiposity and The Polycystic Ovary SyndromeclinicacosimoNessuna valutazione finora
- Aub 15Documento28 pagineAub 15Nadiah Baharum ShahNessuna valutazione finora
- Hormonal Contraception in Women With Polycystic Ovary Syndrome: Choices, Challenges, and Noncontraceptive BenefitsDocumento11 pagineHormonal Contraception in Women With Polycystic Ovary Syndrome: Choices, Challenges, and Noncontraceptive BenefitsMariam QaisNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyDa EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNessuna valutazione finora
- BD Vacutainer Evacuated Blood Collection System - SF - ENDocumento5 pagineBD Vacutainer Evacuated Blood Collection System - SF - ENKopeNessuna valutazione finora
- BC-11 BrochureDocumento2 pagineBC-11 BrochureKopeNessuna valutazione finora
- Spesifikasi - Chem 5Documento1 paginaSpesifikasi - Chem 5KopeNessuna valutazione finora
- Minimal Stimulation Using Letrozole in Poor Responders: Original ArticleDocumento4 pagineMinimal Stimulation Using Letrozole in Poor Responders: Original ArticleKopeNessuna valutazione finora
- Ch. 34 Eoc ReviewDocumento12 pagineCh. 34 Eoc ReviewQussayNessuna valutazione finora
- D2 0905 Paediatric Reference Intervals - An Update - Tina YenDocumento25 pagineD2 0905 Paediatric Reference Intervals - An Update - Tina YenkamalNessuna valutazione finora
- Lecture Quiz On Integumentary SystemDocumento2 pagineLecture Quiz On Integumentary SystemCeline Miller100% (1)
- Female Life CycleDocumento24 pagineFemale Life CycleHenniwidiaa100% (1)
- Adrenal 1 5Documento41 pagineAdrenal 1 5Ditas ChuNessuna valutazione finora
- Calcium Homeostasis: Endocrine Regulation of (Ca)Documento4 pagineCalcium Homeostasis: Endocrine Regulation of (Ca)PRANAB KUMAR MUKHERJEENessuna valutazione finora
- Endocrine SystemDocumento27 pagineEndocrine SystemJustinn DukessaNessuna valutazione finora
- Reaching The Age of AdolescenceDocumento17 pagineReaching The Age of AdolescencevarshavishuNessuna valutazione finora
- Gonadal Hormones and InhibitorsDocumento10 pagineGonadal Hormones and InhibitorsCarlos NiñoNessuna valutazione finora
- Chemical Coordination and IntegrationDocumento8 pagineChemical Coordination and IntegrationJagadesh nvNessuna valutazione finora
- Pathophysiology of DUBDocumento18 paginePathophysiology of DUBAnna San100% (2)
- Glândulas Supra-Renais Ou Adrenais: CórtexDocumento37 pagineGlândulas Supra-Renais Ou Adrenais: CórtexFilipe SilvaNessuna valutazione finora
- 1a ReproductiveAndSexualHealthDocumento2 pagine1a ReproductiveAndSexualHealthKenjie Palaganas CentenoNessuna valutazione finora
- Low Free T4 Normal Free T4 High Free T4Documento3 pagineLow Free T4 Normal Free T4 High Free T4Joseph De JoyaNessuna valutazione finora
- Laporan SPH 2 Sistem ReproduksiDocumento4 pagineLaporan SPH 2 Sistem ReproduksiAghits LailyNessuna valutazione finora
- Control Blood of Calcium LevelsDocumento2 pagineControl Blood of Calcium Levelswoman in stemNessuna valutazione finora
- HyperthyroidismDocumento59 pagineHyperthyroidismjoanna73% (11)
- NCMB 316 Lec Midterm 1Documento14 pagineNCMB 316 Lec Midterm 1zh4hft6pnzNessuna valutazione finora
- Treatment of Pituitary Adenoma by Traditional Medicine TherapiesDocumento3 pagineTreatment of Pituitary Adenoma by Traditional Medicine TherapiesPirasan Traditional Medicine CenterNessuna valutazione finora
- L-02 - Evaluation of Mammary GlandsDocumento30 pagineL-02 - Evaluation of Mammary GlandsNadirAliNessuna valutazione finora
- Journal AnalysisDocumento2 pagineJournal AnalysisJust yor Regular CavegirlNessuna valutazione finora
- Parathyroi D HormoneDocumento25 pagineParathyroi D HormoneChatie PipitNessuna valutazione finora
- Endocrine Nclex QuestionsDocumento9 pagineEndocrine Nclex QuestionsTiffany Fain Noles100% (1)
- Hypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2018 Lectures 1-2 March 14 2018Documento213 pagineHypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2018 Lectures 1-2 March 14 2018rachid09Nessuna valutazione finora
- WEEK 3 Day 1 Lesson 11: Define Menstrual CycleDocumento10 pagineWEEK 3 Day 1 Lesson 11: Define Menstrual Cyclejoice dela cruz100% (1)
- Skin Problems ChartDocumento2 pagineSkin Problems ChartJacqueline Helmy100% (3)
- Harish Kumar Adwani ReportsDocumento3 pagineHarish Kumar Adwani ReportspriyushhospitallabNessuna valutazione finora
- BHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourDocumento2 pagineBHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourzuhaibNessuna valutazione finora
- Endocrine System Quiz 1 PDFDocumento6 pagineEndocrine System Quiz 1 PDFshasagailNessuna valutazione finora
- DR - Ahmed Mowafy - Endocrinology BookDocumento116 pagineDR - Ahmed Mowafy - Endocrinology BookRancesh Famo100% (1)