Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
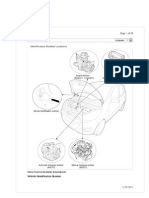
- I10 Workshop Manual - ADocumento292 pagineI10 Workshop Manual - ANorthstartechnology Company82% (11)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Amos FortuneDocumento97 pagineAmos Fortunetongai100% (5)
- Amendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsDocumento2 pagineAmendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsTommy AndersNessuna valutazione finora
- Eric Dollard MWO Update 2012Documento21 pagineEric Dollard MWO Update 2012pic2007100% (7)
- Helminths: NematodesDocumento17 pagineHelminths: NematodesNicolle PanchoNessuna valutazione finora
- 1414-Electric Room 1 Calculation Report Rev.02Documento28 pagine1414-Electric Room 1 Calculation Report Rev.02zakariaelrayesusaNessuna valutazione finora
- Kitchen Colour Ide1Documento6 pagineKitchen Colour Ide1Kartik KatariaNessuna valutazione finora
- Aqa Econ3 QP Jan12Documento8 pagineAqa Econ3 QP Jan12api-247036342Nessuna valutazione finora
- X-Ray Radiation and Gamma RadiationDocumento13 pagineX-Ray Radiation and Gamma RadiationVence MeraNessuna valutazione finora
- Action Plan Gulayan Sa PaaralanDocumento2 pagineAction Plan Gulayan Sa PaaralanAntonio ArienzaNessuna valutazione finora
- Thermal Imaging Tech ResourceDocumento20 pagineThermal Imaging Tech Resourceskimav86100% (1)
- Classification of Tooth StainingDocumento4 pagineClassification of Tooth StainingYAMUNA M.D.S. PAEDODONTICS & PREVENTIVE DENTISTRYNessuna valutazione finora
- Norma ASTM C171Documento2 pagineNorma ASTM C171Jony Gutiérrez100% (1)
- BS en 6100-3-2 Electromagnetic Compatibility (EMC)Documento12 pagineBS en 6100-3-2 Electromagnetic Compatibility (EMC)Arun Jacob CherianNessuna valutazione finora
- MultiCrystallineDataSheet - EN - SilikenDocumento4 pagineMultiCrystallineDataSheet - EN - Silikensydneyaus2005Nessuna valutazione finora
- Kyocera 1800Documento2 pagineKyocera 1800gendoetzNessuna valutazione finora
- 12V-100Ah FTA DatasheetDocumento1 pagina12V-100Ah FTA Datasheetchandrashekar_ganesanNessuna valutazione finora
- 447.010 Screen Operating Manual v001Documento67 pagine447.010 Screen Operating Manual v001José CarlosNessuna valutazione finora
- Electrical Inspections: Infrared ThermographyDocumento28 pagineElectrical Inspections: Infrared ThermographyManish RajNessuna valutazione finora
- Astm A479Documento7 pagineAstm A479Martin RomeroNessuna valutazione finora
- Air Show - Blue Angels in Flying K - The News of NAS KingsvilleDocumento16 pagineAir Show - Blue Angels in Flying K - The News of NAS KingsvilleAlan GuggenheimNessuna valutazione finora
- Heil 4000 FeaturesDocumento1 paginaHeil 4000 FeaturesBogdan NgrNessuna valutazione finora
- Fundamental and Technical Analysis of Iron and Steel SIP PROJECTDocumento34 pagineFundamental and Technical Analysis of Iron and Steel SIP PROJECThaveuever910Nessuna valutazione finora
- Portland PortDocumento18 paginePortland PortAnonymous Lx3jPjHAVLNessuna valutazione finora
- Medical BiotechnologyDocumento4 pagineMedical Biotechnologyعمر بن عليNessuna valutazione finora
- Gummetal Zastosowania Kliniczne 0Documento8 pagineGummetal Zastosowania Kliniczne 0ΑΛΕΞΑΝΔΡΟΣ ΣΤΕΦΑΝΗΣNessuna valutazione finora
- Catálogo DP InglêsDocumento20 pagineCatálogo DP Inglêsjf2003Nessuna valutazione finora
- Ford6000cd Rear ConnectorDocumento2 pagineFord6000cd Rear ConnectorAnonymous WcYW9AeNessuna valutazione finora
- Disorders of The Endocrine System and Dental ManagementDocumento63 pagineDisorders of The Endocrine System and Dental ManagementSanni FatimaNessuna valutazione finora
- Inventory of Flood Bund PunjabDocumento26 pagineInventory of Flood Bund PunjabguildkeyNessuna valutazione finora