Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Letter of IntentDocumento1 paginaLetter of IntentLuz Alpindo Dela CruzNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- SCHEDULEDocumento6 pagineSCHEDULELuz Alpindo Dela CruzNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Apparatus and MaterialsDocumento5 pagineApparatus and MaterialsLuz Alpindo Dela CruzNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- OFFICERSDocumento4 pagineOFFICERSLuz Alpindo Dela CruzNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Experiment 1-2Documento2 pagineExperiment 1-2Luz Alpindo Dela CruzNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Experiment 2Documento34 pagineExperiment 2Luz Alpindo Dela CruzNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- ZOOLOGYDocumento2 pagineZOOLOGYLuz Alpindo Dela CruzNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Exp 1aDocumento8 pagineExp 1aLuz Alpindo Dela CruzNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- CVDC 2018Documento4 pagineCVDC 2018Luz Alpindo Dela CruzNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
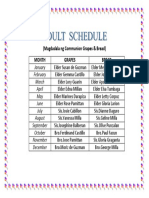
- Grapes & BreadDocumento1 paginaGrapes & BreadLuz Alpindo Dela CruzNessuna valutazione finora
- INSULIN AdministrationDocumento2 pagineINSULIN AdministrationRon LozadaNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Inpatient Glycemic ManagementDocumento13 pagineInpatient Glycemic Managementmiss betawiNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- ACC Handbook Ascvd Type 2 Diabetes: On andDocumento10 pagineACC Handbook Ascvd Type 2 Diabetes: On andZH. omg sarNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Nursing Sample Test 5 Patricia StylesDocumento2 pagineNursing Sample Test 5 Patricia StylesDiana Hazel Delos ReyesNessuna valutazione finora
- Presentation 1Documento6 paginePresentation 1Maya RentinaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Pathophysiology of HypokalemiaDocumento1 paginaPathophysiology of HypokalemiaJessa C. BorjaNessuna valutazione finora
- Diognosa Banding EdemaDocumento1 paginaDiognosa Banding EdemaMargareth SitorusNessuna valutazione finora
- Naihs-Com Mbbs 8 Batch - 2 Year Biochemistry Dr. Jayendra Bajracharya Pre-Lecture Assignment Topic: HypernatremiaDocumento3 pagineNaihs-Com Mbbs 8 Batch - 2 Year Biochemistry Dr. Jayendra Bajracharya Pre-Lecture Assignment Topic: HypernatremiaAlIsh BhanDariNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Study of Antidiabetic Activity of Alli Chooranam (Nymphaea Nouchali) Burm.f)Documento7 pagineStudy of Antidiabetic Activity of Alli Chooranam (Nymphaea Nouchali) Burm.f)IJAR JOURNALNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Group 1 PR2Documento10 pagineGroup 1 PR2Hans Elliza BartocilloNessuna valutazione finora
- Classification of Diabetes Mellitus - Endotext - NCBI BookshelfDocumento11 pagineClassification of Diabetes Mellitus - Endotext - NCBI BookshelfSwati ParijaNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Tight Glycemic Control in Critically Ill PediatricDocumento11 pagineTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNessuna valutazione finora
- The Pancreas: Anatomy and FunctionsDocumento10 pagineThe Pancreas: Anatomy and FunctionsPunx RamoneNessuna valutazione finora
- Project Proposal DiabetesDocumento3 pagineProject Proposal DiabetesShayne Cabotaje Delos Santos - BorlingNessuna valutazione finora
- NURS FPX 5003 Assessment 1 Identifying Community Health NeedsDocumento5 pagineNURS FPX 5003 Assessment 1 Identifying Community Health Needsfarwaamjad771Nessuna valutazione finora
- Patient Care Plan: Nursing Diagnosis (In Priority Order) Patient-Centered Goals Nursing Intervention Rationale EvaluationDocumento3 paginePatient Care Plan: Nursing Diagnosis (In Priority Order) Patient-Centered Goals Nursing Intervention Rationale Evaluationmp1757Nessuna valutazione finora
- Case StudyDocumento4 pagineCase StudyCecil AguilarNessuna valutazione finora
- Hypertension and Diabetes ClubDocumento15 pagineHypertension and Diabetes Clubncd.bulacanNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Acute Complications of Diabetes MellitusDocumento13 pagineAcute Complications of Diabetes MellitusMark Christian M. GonzagaNessuna valutazione finora
- Protocolo Da BombaDocumento52 pagineProtocolo Da BombaEmerson SaNessuna valutazione finora
- IntroductionDocumento13 pagineIntroductionSaadNessuna valutazione finora
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Documento10 pagineDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Artack50% (2)
- Blood Sugar Level Chart: MG/DL General Target RangesDocumento11 pagineBlood Sugar Level Chart: MG/DL General Target RangesbobbymeenaNessuna valutazione finora
- Hesi Gerontology Age-Related Risks PDFDocumento14 pagineHesi Gerontology Age-Related Risks PDFAna BienneNessuna valutazione finora
- Efektivitas Perawatan Luka Dengan Metode Perawatan Luka Modern Dan Perawatan Luka Konvensional Pada Pasien Diabetes MelitusDocumento13 pagineEfektivitas Perawatan Luka Dengan Metode Perawatan Luka Modern Dan Perawatan Luka Konvensional Pada Pasien Diabetes MelitusCitta ChitatoNessuna valutazione finora
- Treatment of Diabetes Using TCMDocumento10 pagineTreatment of Diabetes Using TCMSreekanth KrishnamurthyNessuna valutazione finora
- MECKLENBURG COUNTY PUBLIC HEALTH - SAMPLE Positive COVID-19 Interview QuestionnaireDocumento4 pagineMECKLENBURG COUNTY PUBLIC HEALTH - SAMPLE Positive COVID-19 Interview QuestionnaireWFAENessuna valutazione finora
- Presentation 2Documento46 paginePresentation 2Mark Angelo Picar AbelleraNessuna valutazione finora
- Diabetes Nursing FinalDocumento15 pagineDiabetes Nursing FinalAna Marie Besa Battung-ZalunNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Diabetes Mellitus Nursing Care PlanDocumento7 pagineDiabetes Mellitus Nursing Care PlanVictoria Castillo TamayoNessuna valutazione finora