Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Construction Contract: 1055 Franklin Aye Suite 206 Garden City, Ny 11530 516-308-8517Documento8 pagineConstruction Contract: 1055 Franklin Aye Suite 206 Garden City, Ny 11530 516-308-8517Chloe MorningstarNessuna valutazione finora
- A Phenomenological Study On Social Experience of International Nursing Students in TheirDocumento4 pagineA Phenomenological Study On Social Experience of International Nursing Students in TheirChloe MorningstarNessuna valutazione finora
- Breast Self-Examination Awareness and ComplianceDocumento3 pagineBreast Self-Examination Awareness and ComplianceChloe MorningstarNessuna valutazione finora
- Khaye:: Traction: Is The Act of Pulling or Drawing Which Is Associated With Counter TractionDocumento4 pagineKhaye:: Traction: Is The Act of Pulling or Drawing Which Is Associated With Counter TractionChloe MorningstarNessuna valutazione finora
- Ear ProblemDocumento13 pagineEar ProblemChloe MorningstarNessuna valutazione finora
- Checklist For Newborn: Cavite State UniversityDocumento2 pagineChecklist For Newborn: Cavite State UniversityChloe MorningstarNessuna valutazione finora
- Reimbursement Expense Receipt Reimbursement Expense Receipt: G F N 2 G F N 2 R J R JDocumento4 pagineReimbursement Expense Receipt Reimbursement Expense Receipt: G F N 2 G F N 2 R J R JChloe MorningstarNessuna valutazione finora
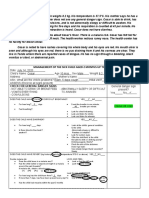
- Management of The Sick Child Aged 2 Months Up To 5 Years: Check For General Danger SignsDocumento4 pagineManagement of The Sick Child Aged 2 Months Up To 5 Years: Check For General Danger SignsChloe MorningstarNessuna valutazione finora
- Management of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarDocumento4 pagineManagement of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarChloe MorningstarNessuna valutazione finora
- Prioritized Problem Date Identified Proposed Project/Action Date Implemented and Status of Implementation (N/A Due To COVID-19)Documento4 paginePrioritized Problem Date Identified Proposed Project/Action Date Implemented and Status of Implementation (N/A Due To COVID-19)Chloe MorningstarNessuna valutazione finora
- Old Signages Around The Institution Assessment/ Observation Management Diagnosis Plans Justification Intervention Resources Evaluation Manpower MaterialsDocumento4 pagineOld Signages Around The Institution Assessment/ Observation Management Diagnosis Plans Justification Intervention Resources Evaluation Manpower MaterialsChloe MorningstarNessuna valutazione finora
- BCG Penta OPV PCV IPV MCV 1 MCV 2 BCG Penta OPV PCV IPV MCV 1 MCV 2Documento1 paginaBCG Penta OPV PCV IPV MCV 1 MCV 2 BCG Penta OPV PCV IPV MCV 1 MCV 2Chloe MorningstarNessuna valutazione finora
- Feeding RecommendationsDocumento1 paginaFeeding RecommendationsChloe MorningstarNessuna valutazione finora
- Filmore CodesDocumento1 paginaFilmore CodesChloe MorningstarNessuna valutazione finora
- Elevated Blood Pressure: Diagnosis Planning Implementation EvaluatonDocumento3 pagineElevated Blood Pressure: Diagnosis Planning Implementation EvaluatonChloe MorningstarNessuna valutazione finora
- College of Nursing Plan of Activities: Collaboration. We Work Collaboratively With Our Clients and Team by Engaging inDocumento3 pagineCollege of Nursing Plan of Activities: Collaboration. We Work Collaboratively With Our Clients and Team by Engaging inChloe MorningstarNessuna valutazione finora
- Cues/Data Nursing Diagnosis Nursing Objectives/Plan Nursing Intervention Nursing EvaluationDocumento1 paginaCues/Data Nursing Diagnosis Nursing Objectives/Plan Nursing Intervention Nursing EvaluationChloe Morningstar100% (1)
- Diocese of Imus Catholic Educational System, Inc. Office of The Superintendent of The Diocesan SchoolsDocumento1 paginaDiocese of Imus Catholic Educational System, Inc. Office of The Superintendent of The Diocesan SchoolsChloe MorningstarNessuna valutazione finora
- INTERPRETATION OneDocumento2 pagineINTERPRETATION OneChloe MorningstarNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 1.2. PTI Insurance Benefits - English VersionDocumento23 pagine1.2. PTI Insurance Benefits - English VersionĐào Duy PhiNessuna valutazione finora
- Iap 2011 PDFDocumento80 pagineIap 2011 PDFnayanastarNessuna valutazione finora
- Pttep Offshore Safety BriefingDocumento50 paginePttep Offshore Safety BriefingRashyd RidhaNessuna valutazione finora
- Roles of Oncology Pharmacists in Korea 20140928Documento17 pagineRoles of Oncology Pharmacists in Korea 20140928adeputra25Nessuna valutazione finora
- Vaccine Wastage Study in Ghana, Mozambique and PakistanDocumento12 pagineVaccine Wastage Study in Ghana, Mozambique and PakistanYee Theng NgNessuna valutazione finora
- All About NailsDocumento16 pagineAll About NailsJoel MarasiganNessuna valutazione finora
- SDG Progress Report Special EditionDocumento43 pagineSDG Progress Report Special EditionSatya VNessuna valutazione finora
- Review of Community DynamicsDocumento41 pagineReview of Community DynamicsDona Kris GumbanNessuna valutazione finora
- Watts New: PCPC For Earth Day: Volunteers Join Trash WalkDocumento9 pagineWatts New: PCPC For Earth Day: Volunteers Join Trash WalkPCPC.PHNessuna valutazione finora
- DS IA EgDocumento7 pagineDS IA Eg赵倞Nessuna valutazione finora
- Lashelle Bennett Sinclair Essay Final DraftDocumento7 pagineLashelle Bennett Sinclair Essay Final Draftapi-519879455Nessuna valutazione finora
- Lecture 5 Research Design Observational Studies (Descriptive and Cross Sectional) - Dr. Dr. Osman Sianipar, DMM., MSC., Sp. PK (K) (2022)Documento49 pagineLecture 5 Research Design Observational Studies (Descriptive and Cross Sectional) - Dr. Dr. Osman Sianipar, DMM., MSC., Sp. PK (K) (2022)Sheila Tirta AyumurtiNessuna valutazione finora
- Discussion Question No 2Documento5 pagineDiscussion Question No 2Vanessa SibayanNessuna valutazione finora
- CHAPTER - 1 - Differential Diagnoses - 2011 - Small Animal Dermatology PDFDocumento21 pagineCHAPTER - 1 - Differential Diagnoses - 2011 - Small Animal Dermatology PDFRanjani RajasekaranNessuna valutazione finora
- Tugas Bahasa Inggris Nama: Yuniarti NPM: 6219111 Kelas: 3ADocumento2 pagineTugas Bahasa Inggris Nama: Yuniarti NPM: 6219111 Kelas: 3AKiki Opo MeneNessuna valutazione finora
- Form 360 March 2020Documento11 pagineForm 360 March 2020shahnawaz100% (1)
- 1, Nurhamlin, Risdayati Dan IndrawatiDocumento15 pagine1, Nurhamlin, Risdayati Dan IndrawatiSophia Amelia PutriNessuna valutazione finora
- MIDTERM Community Nursing 2Documento24 pagineMIDTERM Community Nursing 2Will Garcia100% (2)
- The Impacts of COVID-19 On ChildrenDocumento8 pagineThe Impacts of COVID-19 On ChildrenJosué CastroNessuna valutazione finora
- 1027 Application GuidelineDocumento6 pagine1027 Application GuidelineJORGEALEXERNessuna valutazione finora
- Las Pe10 Day1 Week1 DonnaDocumento4 pagineLas Pe10 Day1 Week1 DonnaBadeth AblaoNessuna valutazione finora
- Annotated BibliographyDocumento5 pagineAnnotated Bibliographyapi-451545971Nessuna valutazione finora
- HS7008 Module Guide T2 - 2019-20Documento14 pagineHS7008 Module Guide T2 - 2019-20OsamaMazhariNessuna valutazione finora
- Daily Dose of Sunshine Case StudyDocumento2 pagineDaily Dose of Sunshine Case Studyvon aliparNessuna valutazione finora
- Human (Science Year 3) - Print - QuizizzDocumento4 pagineHuman (Science Year 3) - Print - QuizizzpiriyachandranNessuna valutazione finora
- Risk Assessment TemplateDocumento3 pagineRisk Assessment TemplateGus VanGeijtenbeekNessuna valutazione finora
- Fabius Plus XLDocumento44 pagineFabius Plus XLAlter DiegoNessuna valutazione finora
- 1 - 030302 - Aqualead MF 880Documento11 pagine1 - 030302 - Aqualead MF 880PoulandeNessuna valutazione finora
- 4SP1Documento2 pagine4SP1Fiona MaligayaNessuna valutazione finora
- Content: Standard Operating Procedure (SOP) Use and Maintenance of An AutoclaveDocumento10 pagineContent: Standard Operating Procedure (SOP) Use and Maintenance of An Autoclaverijulesh karmelNessuna valutazione finora