Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- ACR 2018 TXIT Exam RationalesDocumento94 pagineACR 2018 TXIT Exam Rationalesgermanfutbol7100% (3)
- ANA Recognized Terminologies and Data Element SetsDocumento5 pagineANA Recognized Terminologies and Data Element SetsBlair WoodsenNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Care of Mother, Child, Adolescent (Autosaved)Documento23 pagineCare of Mother, Child, Adolescent (Autosaved)Shing Mae Marie100% (10)
- Knee Anatomy PDFDocumento11 pagineKnee Anatomy PDFDr.Ammar MasoodNessuna valutazione finora
- Hioerplasia Mamaria GestacionalDocumento9 pagineHioerplasia Mamaria GestacionalOctavio LeyvaNessuna valutazione finora
- Legislations Clinical Rights and Professional ResponsibilityDocumento10 pagineLegislations Clinical Rights and Professional ResponsibilityFarheen khanNessuna valutazione finora
- Breast Engrogement FinalDocumento41 pagineBreast Engrogement FinalSharmistha DebnathNessuna valutazione finora
- Instrumental Analysis of Swallowing - PDF / KUNNAMPALLIL GEJODocumento65 pagineInstrumental Analysis of Swallowing - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNessuna valutazione finora
- Ethicon Harmonic 300 Ultrasonic Surgery Generator - User ManualDocumento36 pagineEthicon Harmonic 300 Ultrasonic Surgery Generator - User Manualreinahr100% (1)
- Catherineresume 2Documento3 pagineCatherineresume 2api-302133133Nessuna valutazione finora
- Increased ICP & ICSDocumento69 pagineIncreased ICP & ICSSan ShineNessuna valutazione finora
- Maternity Benefits Requirements DocsDocumento2 pagineMaternity Benefits Requirements DocsGladys April CatarojaNessuna valutazione finora
- Synactive Theory of Newborn Behavioral Organization and Development - WikipediaDocumento14 pagineSynactive Theory of Newborn Behavioral Organization and Development - WikipediaYuseva SariatiNessuna valutazione finora
- University of Veterinary and Animal Sciences - Lahore: Controller OfficeDocumento1 paginaUniversity of Veterinary and Animal Sciences - Lahore: Controller OfficeVet IrfanNessuna valutazione finora
- Pediatrics 2002 Ballard E63Documento8 paginePediatrics 2002 Ballard E63dentistalitNessuna valutazione finora
- Asha Monthly Reports - Aprial MonthDocumento64 pagineAsha Monthly Reports - Aprial MonthSamuel SourabNessuna valutazione finora
- Medical Abbreviations A-ZDocumento5 pagineMedical Abbreviations A-ZTrixie GulokNessuna valutazione finora
- HYPERALDOSTERONISMDocumento7 pagineHYPERALDOSTERONISMMarnee Justine ColladoNessuna valutazione finora
- Obstetrics OBDocumento65 pagineObstetrics OBVicviclookTheking100% (1)
- Chnn211 Lec (Philippine Health Care Delivery System) : The PhilippinesDocumento6 pagineChnn211 Lec (Philippine Health Care Delivery System) : The Philippineskristelaaa guevarraNessuna valutazione finora
- Tahbso ArticleDocumento4 pagineTahbso ArticleAlianna Kristine OhNessuna valutazione finora
- Histology of Oral Mucous Membrane and GingivaDocumento86 pagineHistology of Oral Mucous Membrane and GingivahazeemmegahedNessuna valutazione finora
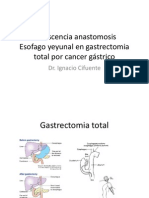
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocumento22 pagineDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooNessuna valutazione finora
- Vascular Surgery OsceDocumento66 pagineVascular Surgery Osceapi-19579909233% (3)
- Small Animal Maternal Behavior and Its AberrationsDocumento4 pagineSmall Animal Maternal Behavior and Its AberrationsPablo Herreros UbaldeNessuna valutazione finora
- The Uses and Limitations of The Fetal Biophysical Profile.Documento18 pagineThe Uses and Limitations of The Fetal Biophysical Profile.Diego Ortecho100% (1)
- Kandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Documento14 pagineKandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Zarif SyafiqNessuna valutazione finora
- Requirements and Prosedures Under Act 586Documento124 pagineRequirements and Prosedures Under Act 586Sazynrash ManogaranNessuna valutazione finora
- SURGICAL CARE COMPLEX POLICY (OsMak-CLN-SD-SCC) PDFDocumento2 pagineSURGICAL CARE COMPLEX POLICY (OsMak-CLN-SD-SCC) PDFpatientsafetyNessuna valutazione finora
- Liceo NavalDocumento6 pagineLiceo NavalEdgart A. Alfaro100% (1)