Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Effectiveness of Facebook As An Advertisement Platform-Desiree D. FrancoDocumento28 pagineThe Effectiveness of Facebook As An Advertisement Platform-Desiree D. FrancoDesiree FrancoNessuna valutazione finora
- How To Fight Presidents by Daniel O'Brien - ExcerptDocumento8 pagineHow To Fight Presidents by Daniel O'Brien - ExcerptCrown Publishing Group100% (1)
- Detailed Lesson Plan in Health (Final Demo)Documento4 pagineDetailed Lesson Plan in Health (Final Demo)Maria Gizella Valencia Paa80% (71)
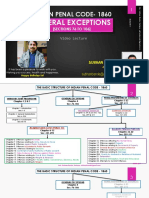
- IPC Part-II PDFDocumento38 pagineIPC Part-II PDFHarsh Vardhan Singh HvsNessuna valutazione finora
- Prospectus FKP Curacao 1Documento18 pagineProspectus FKP Curacao 1于博文Nessuna valutazione finora
- Activity-Sheets-ENGLISH 6 QUARTER 4 W5-8Documento13 pagineActivity-Sheets-ENGLISH 6 QUARTER 4 W5-8grace budumo mosqueda100% (1)
- Coast Guard CredoDocumento1 paginaCoast Guard CredoKenneth John Jayme56% (9)
- Lrmds Action Plan 2018Documento1 paginaLrmds Action Plan 2018Ling Pau0% (1)
- Zara Case Study PDFDocumento2 pagineZara Case Study PDFMoiz MunisNessuna valutazione finora
- Abayon Vs HretDocumento2 pagineAbayon Vs HretKenneth John Jayme75% (4)
- Birthday March EnvelopeDocumento4 pagineBirthday March EnvelopeKenneth John JaymeNessuna valutazione finora
- Rooster For CmcpoDocumento1 paginaRooster For CmcpoKenneth John JaymeNessuna valutazione finora
- Administrative Law Case DigestDocumento11 pagineAdministrative Law Case DigestKenneth John JaymeNessuna valutazione finora
- IV. Principles of Construction B.general Principles or Presumptions On The Interpretation of Certain StatutesDocumento24 pagineIV. Principles of Construction B.general Principles or Presumptions On The Interpretation of Certain StatutesKenneth John JaymeNessuna valutazione finora
- Arguments in Favour of CSRDocumento7 pagineArguments in Favour of CSRDani Sha100% (2)
- Receive and Process Reservations in Hotel and Travel IndustriesDocumento68 pagineReceive and Process Reservations in Hotel and Travel IndustriesChin DhoNessuna valutazione finora
- Gmail - Bus Ticket - Bhopal To Sagar On Thu, 15 Aug 2019 and Rate Your ExperienceDocumento4 pagineGmail - Bus Ticket - Bhopal To Sagar On Thu, 15 Aug 2019 and Rate Your ExperienceShivamSrivastavaNessuna valutazione finora
- Savitribai Phule Pune University: Timetable For Backlog & Performance Improvement Online Examination of APR/MAY 2020Documento11 pagineSavitribai Phule Pune University: Timetable For Backlog & Performance Improvement Online Examination of APR/MAY 2020Daveed starkNessuna valutazione finora
- A STUDY ON QUALITY OF WORK LIFE OF EMPLOYEES IN PARAGON STEELS PVT LTD KANJIKODE C 1210Documento3 pagineA STUDY ON QUALITY OF WORK LIFE OF EMPLOYEES IN PARAGON STEELS PVT LTD KANJIKODE C 1210Gokul S DasNessuna valutazione finora
- For SouvenirDocumento1 paginaFor SouvenirKarizza Zoette Ann AlcardeNessuna valutazione finora
- M - A - (Journalism & Mass Communication) - 309 12 - Evolution of Media PDFDocumento212 pagineM - A - (Journalism & Mass Communication) - 309 12 - Evolution of Media PDFdev rs100% (1)
- Activity Sheet in Business Enterprise SimulationDocumento4 pagineActivity Sheet in Business Enterprise SimulationAimee LasacaNessuna valutazione finora
- Latihan Soal Schedule: Read The Following Text To Answer Questions Number 1 and 2Documento6 pagineLatihan Soal Schedule: Read The Following Text To Answer Questions Number 1 and 2Ibu ErniNessuna valutazione finora
- History of Cooperative in The PhilippinesDocumento21 pagineHistory of Cooperative in The PhilippinesNichole MendozeNessuna valutazione finora
- Global E-Business: How Businesses Use Information SystemsDocumento34 pagineGlobal E-Business: How Businesses Use Information SystemsFahim MahmudNessuna valutazione finora
- Daily Lesson Plan: No Name Disability AttendanceDocumento7 pagineDaily Lesson Plan: No Name Disability AttendanceebellaamayrahaisyahNessuna valutazione finora
- Juvenile A Subject To Be Scrutinize Socio AssignmentDocumento20 pagineJuvenile A Subject To Be Scrutinize Socio AssignmentmitukpanwarNessuna valutazione finora
- ICA - 1996-09-06 - Code of Ethics - EN PDFDocumento3 pagineICA - 1996-09-06 - Code of Ethics - EN PDFLulu MiticaNessuna valutazione finora
- AB CAIIB Paper 1 Module C Human Resource Management PDFDocumento29 pagineAB CAIIB Paper 1 Module C Human Resource Management PDFdilipNessuna valutazione finora
- Check List - Product Realisation ProcessDocumento4 pagineCheck List - Product Realisation ProcessDisha ShahNessuna valutazione finora
- Synopsis On Shopping Mall Essay - 1127 WordsDocumento10 pagineSynopsis On Shopping Mall Essay - 1127 WordsShivam AroraNessuna valutazione finora
- ESU Mauritius Newsletter Dec 09Documento4 pagineESU Mauritius Newsletter Dec 09esumauritiusNessuna valutazione finora
- Milk Tea Industry: An Exploratory Study: February 2020Documento9 pagineMilk Tea Industry: An Exploratory Study: February 2020NING ANGELNessuna valutazione finora
- Ngo Quoc Tuan - HR Executive - CVDocumento3 pagineNgo Quoc Tuan - HR Executive - CVThanh DangNessuna valutazione finora
- Fatal Charades Roman Executions Staged AsDocumento33 pagineFatal Charades Roman Executions Staged AsMatheus Scremin MagagninNessuna valutazione finora
- Iso 9001 TemplateDocumento2 pagineIso 9001 Templatefranckri3010Nessuna valutazione finora