Potrebbero piacerti anche
- Hemolytic Disease of The Newborn: (Erythroblastosis Fetalis)Documento17 pagineHemolytic Disease of The Newborn: (Erythroblastosis Fetalis)sandeepv08Nessuna valutazione finora
- Cyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsValutazione: 5 su 5 stelle5/5 (1)
- Prevalence of Protein Energy Malnutrition Among UnderDocumento6 paginePrevalence of Protein Energy Malnutrition Among UnderagungNessuna valutazione finora
- Adrenal InsufficiencyDocumento33 pagineAdrenal InsufficiencypukitagabNessuna valutazione finora
- Discharge Plan EndoDocumento3 pagineDischarge Plan EndoCharlayne AnneNessuna valutazione finora
- g6pd BrochureDocumento2 pagineg6pd BrochureMaha GaberNessuna valutazione finora
- Hematology & Immune SystemDocumento81 pagineHematology & Immune SystemAmanuel Maru100% (1)
- Pathophysiology of Uterine FibroidsDocumento14 paginePathophysiology of Uterine FibroidsRANessuna valutazione finora
- Nephrotic Syndrome Anak LapkasDocumento32 pagineNephrotic Syndrome Anak LapkasChristy SitorusNessuna valutazione finora
- Celiac Disease: An Autoimmune Condition Triggered by GlutenDocumento2 pagineCeliac Disease: An Autoimmune Condition Triggered by GlutenGiabellNessuna valutazione finora
- KwashiorkorDocumento4 pagineKwashiorkorreshma banuNessuna valutazione finora
- DiarrheaDocumento38 pagineDiarrheaSTEPHANIE SOR100% (1)
- Bartter Syndrome: Rare Inherited Kidney DisorderDocumento3 pagineBartter Syndrome: Rare Inherited Kidney DisorderEnny Andriani100% (1)
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocumento44 paginePractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNessuna valutazione finora
- Congenital Adrenal HyperplasiaDocumento29 pagineCongenital Adrenal HyperplasiaMohan RaoNessuna valutazione finora
- Update On Cancer CachexiaDocumento4 pagineUpdate On Cancer CachexiaIyanNessuna valutazione finora
- Case Study Anemia-1Documento6 pagineCase Study Anemia-1Melsya H UtamiNessuna valutazione finora
- Anemia in ChildrenDocumento4 pagineAnemia in ChildrenTeslim Raji100% (1)
- Henoch Schonlein Purpura REVDocumento42 pagineHenoch Schonlein Purpura REVBayu Kurniawan100% (1)
- Biliary DyskinesiaDocumento1 paginaBiliary DyskinesiaYolotl Hilario Sanchez CarrilloNessuna valutazione finora
- Biochemistry of GlycoproteinDocumento6 pagineBiochemistry of GlycoproteinMahathir Mohmed100% (7)
- Approach To The Child With Anemia - UpToDateDocumento41 pagineApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasNessuna valutazione finora
- Acute Appendicitis in ChildrenDocumento71 pagineAcute Appendicitis in ChildrenMohamed KamaraNessuna valutazione finora
- The Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021Documento6 pagineThe Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021International Journal of Innovative Science and Research Technology100% (1)
- Theory UrinalysisDocumento23 pagineTheory UrinalysisAnggi Dyah AristiNessuna valutazione finora
- Scrotal HerniaDocumento9 pagineScrotal HerniaReymart BolagaoNessuna valutazione finora
- Free Radical Theory of AgingDocumento2 pagineFree Radical Theory of AgingJenny Rose Colico RNNessuna valutazione finora
- Hematologic DisordersDocumento197 pagineHematologic DisordersDanica Mae BianitoNessuna valutazione finora
- CHILD MALNUTRITIONDocumento59 pagineCHILD MALNUTRITIONflex gy100% (1)
- Anemia in CKDDocumento149 pagineAnemia in CKDUlises ContrerasNessuna valutazione finora
- Opd CaseDocumento13 pagineOpd CaseRaven CièlNessuna valutazione finora
- Measles Virus Case StudyDocumento12 pagineMeasles Virus Case StudyElena Cibu100% (1)
- Emergency Care (Hemophilia)Documento30 pagineEmergency Care (Hemophilia)Nica Georgelle Maniego SamonteNessuna valutazione finora
- UtiDocumento38 pagineUtiAzra AzmunaNessuna valutazione finora
- Sheehan SyndromeDocumento6 pagineSheehan SyndromeArvie TagnongNessuna valutazione finora
- A Case Study of Epidural HematomaDocumento27 pagineA Case Study of Epidural HematomaNeil GoNessuna valutazione finora
- Diarrhea 2016Documento37 pagineDiarrhea 2016oli garkiNessuna valutazione finora
- Pku AlkDocumento33 paginePku AlkSharf WangNessuna valutazione finora
- Case Report Pediatric Von&JepDocumento23 pagineCase Report Pediatric Von&JepFarizan NurmushoffaNessuna valutazione finora
- Diabetes MilletusDocumento31 pagineDiabetes MilletusMary Joy SumandaNessuna valutazione finora
- Neonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamageDocumento6 pagineNeonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamagemuzamirNessuna valutazione finora
- Nephrotic Syndrome ManagementDocumento6 pagineNephrotic Syndrome ManagementRagabi RezaNessuna valutazione finora
- Glucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationDocumento2 pagineGlucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationJinky TenezaNessuna valutazione finora
- Renal Case Study Final-2Documento7 pagineRenal Case Study Final-2api-295221163100% (1)
- Acute Appendicitis Learning LogDocumento10 pagineAcute Appendicitis Learning Logsuman subediNessuna valutazione finora
- POLYCYTHEMIADocumento29 paginePOLYCYTHEMIAFaizan KhanNessuna valutazione finora
- DIC Case StudyDocumento7 pagineDIC Case StudyRobertNessuna valutazione finora
- Paediatric Diabetic KetoacidosisDocumento7 paginePaediatric Diabetic KetoacidosisJuan Carlos BayonaNessuna valutazione finora
- Stevens Johnson DiseaseDocumento5 pagineStevens Johnson DiseaseShammy RNNessuna valutazione finora
- Hypoxia and CyanosisDocumento33 pagineHypoxia and CyanosisRamlah IbrahimNessuna valutazione finora
- Aklan State University Nursing Readings on Pyloric StenosisDocumento5 pagineAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
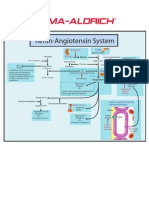
- Renin-Angiotensin SystemDocumento1 paginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Hepatitis overview and nursing careDocumento18 pagineHepatitis overview and nursing careAnne B. BuenvenidaNessuna valutazione finora
- Koch's PostulatesDocumento1 paginaKoch's PostulatesJonathan ChuaNessuna valutazione finora
- Manual 24 Hour RecallDocumento160 pagineManual 24 Hour RecallMadalina CervidNessuna valutazione finora
- Semen Analysis - Purpose, Procedure & ResultsDocumento3 pagineSemen Analysis - Purpose, Procedure & ResultsMotaqiNessuna valutazione finora
- Types of MalnutritionDocumento8 pagineTypes of Malnutritionkazz!Nessuna valutazione finora
- Ma RasmusDocumento13 pagineMa RasmuswekkudeweNessuna valutazione finora
- Chapter 12. Protein-Energy Malnutrition: Causes and EpidemiologyDocumento14 pagineChapter 12. Protein-Energy Malnutrition: Causes and EpidemiologyIrma KurniawatiNessuna valutazione finora
- Wjem 18 487Documento9 pagineWjem 18 487Gesa Syauqi HumairaNessuna valutazione finora
- Jurnal PRP 1-IndraDocumento7 pagineJurnal PRP 1-IndraGesa Syauqi HumairaNessuna valutazione finora
- Jurnal PRP 10-IndraDocumento3 pagineJurnal PRP 10-IndraGesa Syauqi HumairaNessuna valutazione finora
- Bab 125 Glomerulonefritis PDFDocumento4 pagineBab 125 Glomerulonefritis PDFGesa Syauqi HumairaNessuna valutazione finora
- Referensi DA 10-LitaDocumento22 pagineReferensi DA 10-LitaGesa Syauqi HumairaNessuna valutazione finora
- Referensi DA 1-LitaDocumento10 pagineReferensi DA 1-LitaGesa Syauqi HumairaNessuna valutazione finora
- 4Documento22 pagine4Gesa Syauqi HumairaNessuna valutazione finora
- Visum Mati Trisakti ADocumento8 pagineVisum Mati Trisakti AGesa Syauqi HumairaNessuna valutazione finora
- Mind Map IKM - Gesa 03013082Documento10 pagineMind Map IKM - Gesa 03013082Gesa Syauqi HumairaNessuna valutazione finora
- Open Fractures - OrthoInfo - AAOSDocumento10 pagineOpen Fractures - OrthoInfo - AAOSGesa Syauqi HumairaNessuna valutazione finora
- Lupus Erythematosus Fitzpatrick 9Documento22 pagineLupus Erythematosus Fitzpatrick 9Gesa Syauqi HumairaNessuna valutazione finora
- Best Makeup Remover - Penelusuran GoogleDocumento1 paginaBest Makeup Remover - Penelusuran GooglettsyyyaaNessuna valutazione finora
- Revision Oral Pathology: Dr. Nermine El BaheyDocumento58 pagineRevision Oral Pathology: Dr. Nermine El BaheyEslam abokhalilNessuna valutazione finora
- Basic Skin Lesions: Presented By: Dr. Divyank A. Vankawala Jr. Resident, Dermatology Dept., NDMVPS VP Medical CollegeDocumento46 pagineBasic Skin Lesions: Presented By: Dr. Divyank A. Vankawala Jr. Resident, Dermatology Dept., NDMVPS VP Medical CollegeniveditakartikNessuna valutazione finora
- Endorse Data DiniDocumento2 pagineEndorse Data DiniDini AurelitaNessuna valutazione finora
- Scarless Silicone Gel BrochureDocumento6 pagineScarless Silicone Gel BrochureKhaled SalahNessuna valutazione finora
- What Is A RashDocumento8 pagineWhat Is A RashJudi Ann MagsacayNessuna valutazione finora
- Skin Disorder PBCDocumento6 pagineSkin Disorder PBCRatusweethella Intan Yudagrahania PuspitaNessuna valutazione finora
- Diploma in Cosmetology - Clinical & AyurvedicDocumento2 pagineDiploma in Cosmetology - Clinical & AyurvedicJdNessuna valutazione finora
- Superficial Fungal Disorders of The SkinDocumento121 pagineSuperficial Fungal Disorders of The SkinhaniNessuna valutazione finora
- CD ListDocumento80 pagineCD ListOFC accountNessuna valutazione finora
- Eritro Papulo Skuamosa 2021Documento47 pagineEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Cellulitis Talk Jan 2018Documento16 pagineCellulitis Talk Jan 2018Ramsyifa VirzanisdaNessuna valutazione finora
- What Are The Symptoms of Scabies?: For More Information About Scabies, VisitDocumento1 paginaWhat Are The Symptoms of Scabies?: For More Information About Scabies, VisitMuhammad ZaineNessuna valutazione finora
- Harvard Referencing: Guide: (Please Note: This Document Was Downloaded From Citethisforme Web Tool, URL )Documento13 pagineHarvard Referencing: Guide: (Please Note: This Document Was Downloaded From Citethisforme Web Tool, URL )Benjamin K JaravazaNessuna valutazione finora
- Contact Nummular (Discoid) Eczema From Depilating Cream: Case ReportDocumento2 pagineContact Nummular (Discoid) Eczema From Depilating Cream: Case ReportMorindaNessuna valutazione finora
- Scabies - Epidemiology, Clinical Features, and Diagnosis - UpToDateDocumento61 pagineScabies - Epidemiology, Clinical Features, and Diagnosis - UpToDateJorge ArcentalesNessuna valutazione finora
- Blistering DisordersDocumento34 pagineBlistering DisordersSucdi CabdiNessuna valutazione finora
- BSBMED301: Assessment 3: What You Have To DoDocumento9 pagineBSBMED301: Assessment 3: What You Have To DoemilyNessuna valutazione finora
- HH 7Documento2 pagineHH 7CHENNAM PRAVEENNessuna valutazione finora
- Toronto Notes DermatologyDocumento52 pagineToronto Notes Dermatologyalphabeta101100% (1)
- Derma BriefDocumento7 pagineDerma BriefjeharatNessuna valutazione finora
- Treatment of Skin Disease Comprehensive Therapeutic Strategies 5th EditionDocumento62 pagineTreatment of Skin Disease Comprehensive Therapeutic Strategies 5th Editionbetty.washington515100% (36)
- Doctor provides concise SEO-optimized titles for social media postsDocumento3 pagineDoctor provides concise SEO-optimized titles for social media postsAmalia OseacaNessuna valutazione finora
- How to look 「皮疹」Documento50 pagineHow to look 「皮疹」Satoshi KobayashiNessuna valutazione finora
- Genital Nevus PresentationDocumento18 pagineGenital Nevus PresentationdaveNessuna valutazione finora
- Herpes Simplex ReportDocumento17 pagineHerpes Simplex ReportRoxanne Postrano De VeraNessuna valutazione finora
- Acne Eczema Scabies 2014Documento22 pagineAcne Eczema Scabies 2014Novita Dwi MardiningtyasNessuna valutazione finora
- Invoice Original Care Trading CompanyDocumento2 pagineInvoice Original Care Trading CompanyAbdoalhadi AbduallahNessuna valutazione finora
- The Ultimate Beginners Guide To SkincareDocumento65 pagineThe Ultimate Beginners Guide To SkincareSarievoNessuna valutazione finora
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocumento95 pagineBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiNessuna valutazione finora
- Keto Friendly Recipes: Easy Keto For Busy PeopleDa EverandKeto Friendly Recipes: Easy Keto For Busy PeopleValutazione: 3.5 su 5 stelle3.5/5 (2)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDa EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisValutazione: 3 su 5 stelle3/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomDa EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomValutazione: 4 su 5 stelle4/5 (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDa EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyValutazione: 5 su 5 stelle5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellDa EverandForever Strong: A New, Science-Based Strategy for Aging WellNessuna valutazione finora
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsDa EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsValutazione: 4 su 5 stelle4/5 (49)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthDa EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthValutazione: 5 su 5 stelle5/5 (37)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodDa EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodValutazione: 4.5 su 5 stelle4.5/5 (18)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItDa EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItValutazione: 4.5 su 5 stelle4.5/5 (19)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingDa EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingValutazione: 5 su 5 stelle5/5 (59)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainDa EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainValutazione: 3.5 su 5 stelle3.5/5 (6)
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthDa EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthValutazione: 4 su 5 stelle4/5 (7)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDa EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNessuna valutazione finora
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouDa EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNessuna valutazione finora
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDa EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookValutazione: 3.5 su 5 stelle3.5/5 (2)
- Summary of Mary Claire Haver's The Galveston DietDa EverandSummary of Mary Claire Haver's The Galveston DietValutazione: 5 su 5 stelle5/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreDa EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreValutazione: 5 su 5 stelle5/5 (17)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeDa EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeValutazione: 5 su 5 stelle5/5 (1)
- The Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodDa EverandThe Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodValutazione: 4.5 su 5 stelle4.5/5 (20)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeDa EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeValutazione: 4 su 5 stelle4/5 (3)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthDa EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNessuna valutazione finora
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodDa EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodValutazione: 2 su 5 stelle2/5 (1)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondDa EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondValutazione: 4.5 su 5 stelle4.5/5 (28)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossDa EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossValutazione: 4 su 5 stelle4/5 (22)
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanDa EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanValutazione: 3.5 su 5 stelle3.5/5 (3)
- The Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITDa EverandThe Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITValutazione: 5 su 5 stelle5/5 (1)
- Kintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritDa EverandKintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritValutazione: 4.5 su 5 stelle4.5/5 (3)
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossDa EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossValutazione: 4.5 su 5 stelle4.5/5 (22)